
A new generation of API-based interoperability standards is emerging. In contrast to traditional interface specifications, these new approaches focus on reuse of standardized APIs and other “building blocks” which can often be re-combined to address new high-level use-cases without requiring a “start from scratch” for each new use-case.
API access to Health IT systems is not new, but following the JASON report and the JASON Task Force recommendations to the HIT Standards and Policy Committees, there is growing interest into a standards-based API that could become widely supported across many kinds of Health IT. One particular emerging standard, HL7’s Fast Healthcare Interoperability Resources (FHIR) shows promise as becoming a widely supported standard. Vendors and some large provider groups have created the Argonaut Project to define and publish implementation guides in an effort to standardize FHIR implementations across the Health IT community. The FHIR standard specifies many low-level data access services that can be used as “building blocks” to assemble more complex interoperability functionality.
API-based approaches to interoperability have the advantage that APIs can be assembled to rapidly create different kinds of aggregate functions. However, API-based interoperability still requires attention to important implementation details, similar to traditional interoperability specifications. In particular, given the flexibility of APIs, an API-based approach will need to address many required and optional constraints that are necessary to support a desired use-case. For example, if using FHIR as the base API specification, here are some of the constraints that should be considered:
- Which specific data resources are required for the intended interoperability use-case (e.g., patient, encounter, observation)?
- For each resource, what constraints are placed on the values that are allowed for the resource’s data elements (e.g., LOINC, SNOMED)?
- What transport will be used to move the resources back and forth (e.g., HTTP, batch files)?
- Which API operations (e.g. GET (read), PUT (write)) are required?
- For each operation, what operational parameters are required (e.g., supported query parameters for GET)?
- What security model is used to handle authentication, authorization, and encryption (e.g., OAuth, TLS)?
- What other standards are necessary for the overall use-case to be deployed (e.g., HTML, JSON, etc.)?
A specific API-based interoperability use-case will probably need to specify, in the form of an implementation specification, most of the above categories. Some API standards, such as FHIR, contain formal mechanisms (Profiles, Conformance Statements) for specifying constraints, though even a comprehensive specification like FHIR will require that some of the constraints are documented outside of the standard’s formal tools.
To give a more concrete example, consider the “SMART on FHIR” interoperability specification. SMART on FHIR defines a mechanism for interoperable “SMART Apps” that can be plugged in to EHRs and other Health IT systems. Each SMART App can expose a user interaction, and can access data in the underlying system. This presents a powerful way to extend EHR capabilities via “pluggable” app functionality. Dozens of SMART apps are available, with more expected in the future. These apps serve many different clinical needs, yet they all use the same underlying FHIR-based API functionality. However, even though SMART apps are all based on the FHIR standard, it’s not sufficient to simply say “use FHIR”. Here are some of the additional specifications that are needed:
- Resources – Which FHIR resources are available to the App developer? Many EHR vendors are choosing to expose some of the resources defined in ONC’s 2015 Edition Health IT Certification Criteria API requirement. Typical resources available include: Patient, Encounter, Condition, Observation, etc. Not all vendors will elect to expose the exact same set of resources, and some apps may require resources that are not contained in the 2015 Certification list, such as Schedule.
- Resource Profiles – For each supported resource, the FHIR implementation will follow some Profile that specifies how the data fields in the resource will be populated. The Profile will usually define the cardinality of the data (zero, one, or many instances allowed) as well as the Value Sets supported (e.g., LOINC, SNOMED, RxNorm, etc.) Note that formal use of FHIR Profiles is not widely supported at present, so the data constraints are often documented via spreadsheet or other informal means.
- Transport – SMART Apps use HTTP as the transport since they are designed to be interactive and need real-time access to EHR data. The FHIR specification contains a clear mapping of standard data operations (read, write, update, etc.) to the standard HTTP verbs (PUT, GET, etc.)
- API Operations – The 2015 Certification specification currently requires that EHRs support “read only” operations, using the HTTP GET operation. Some vendors have begun to support selected “write” operations using POST, PUT, or UPDATE. Note that the supported write operations may apply only to certain resources. For example, an app might be able to PUT a new Observation, but not be allowed to PUT a new Encounter.
- Parameters – for each resource and operation, the interoperability specification will need to specify which data access parameters are supported. Typically, these include the types of query functions supported by the GET operation. For example, some implementation will support “GET Patient” using the patient’s medical record number, but might not support a “GET Patient” using the SSN or a hospital room number.
- Security Model – The SMART on FHIR specification makes heavy use of the OAuth 2 security standard to orchestrate the HTTP transactions. OAuth may be combined with OpenID Connect in order to cover both authentication and authorization. HTTPS (TLS) is required for on-the-wire encryption. Note that the OAuth 2 standard (which is managed by the IETF) requires its own implementation guide to constrain it for healthcare uses.
- Other Standards – SMART Apps can use HTML5 to control the visual expression of the app, so in some sense, HTML5 is part of the overall specification for SMART on FHIR.
- Trust Relationship – For interoperability using FHIR to work, a trust relationship must be established between entities (ie an EHR/clinical system and an app). This is currently being accomplished by establishing siloed ecosystems. Without an established trust relationship, access to information is not possible regardless of the standards used.
This example illustrates that even though API-based interoperability enables powerful new approaches, there is still a need to carefully specify and constrain each layer of the overall interface orchestration in order to achieve the desired degree of standardization and interoperability.
Text developed by the Health IT Standards Committee as part of the 2017 ISA Task Force
NCPDP Connectivity Operating Rules Implementation Guide an API Application Programming
NCPDP Connectivity Operating Rules Implementation Guide - “An API – application programming interface – at its most basic level, allows your product or service to talk to other products or services. In this way, an API allows you to open up data and functionality to other developers and to other businesses. It is increasingly the way in which agencies and companies exchange data and services, both internally and externally”. There are common technical and practical choices companies need to be aware of when using APIs. This document lays out some of the requirements to ensure the NCPDP Standards employ the API standards appropriately.
For details, refer to the Connectivity Operating Rules Implementation Guide at NCPDP Standards (https://standards.ncpdp.org/Access-to-Standards.aspx).
Help
1. Optional: Background Text / Cover Letter
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
This field is entirely optional and serves the following purposes:
- Provides context for reviewers
- Serves as an introduction if submitting multiple comments
- Functions as a cover letter for formal submissions
If you are submitting a single comment for a specific data class or element, you may leave this field blank. For multiple comments, this space is useful for explaining the overall purpose or connection between your comments.
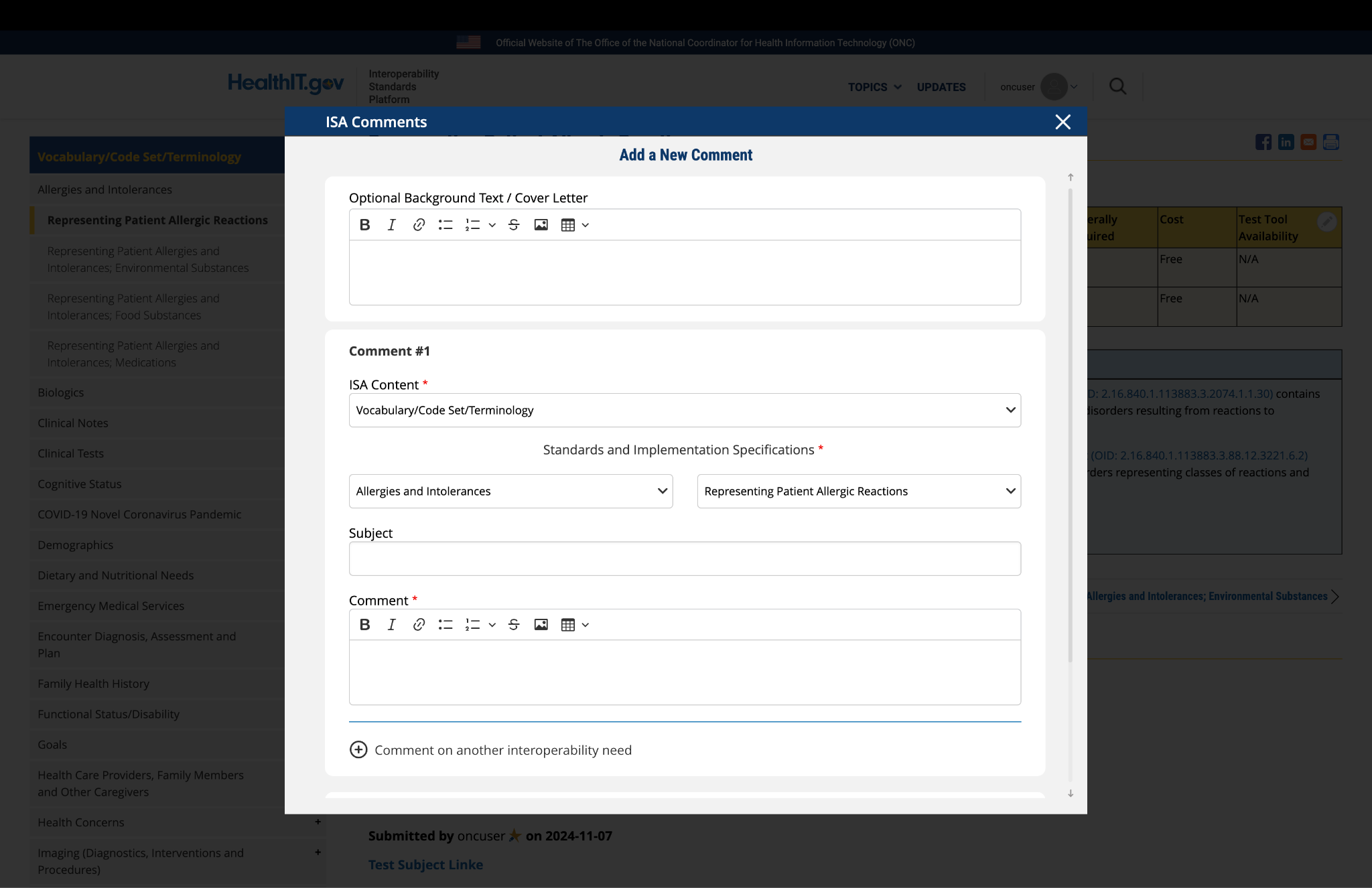
Fig 1 The "Optional Background Text / Cover Letter" field allows users to provide contextual information or introductory remarks for their comment submission.
2. Complete the Comment Form
The comment form contains several fields that require your input:
ISA Content: This field is automatically populated based on the page you are currently viewing. No action is required.
Standards and Implementation Specifications: This drop-down menu is pre-selected based on the topic you're commenting on. The selection reflects the relevant standard or implementation specification for your current page.
Subject: Enter a concise title that summarizes the focus of your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: This is the main field where you provide your detailed feedback, concerns, or suggestions. The comment box includes a text editor with formatting options that allow you to:
- Format text as bold or italic
- Insert hyperlinks
- Create bullet points
- Create numbered lists
- Apply strike-through formatting
- Attach images
- Insert tables
Use these formatting options as needed to clearly present your information.

Fig 2 The comment text editor toolbar provides formatting options including bold, italic, links, lists, tables, and image insertion capabilities.
3. Optional: Add Additional Comments
If you need to provide feedback on multiple aspects of the ISA content, you can add additional comments:
- After completing your first comment, locate and click the link labeled "Comment on another interoperability need" at the bottom of the form.
- A new comment section will appear, allowing you to enter details for your additional comment.
- For this new comment section, the "ISA Content" and "Standards and Implementation Specifications" fields will not be automatically populated. You must select the appropriate content and specification from the drop-down menus for each additional comment.
- Complete all required fields for your additional comment.
- Repeat this process for each additional comment you wish to submit.
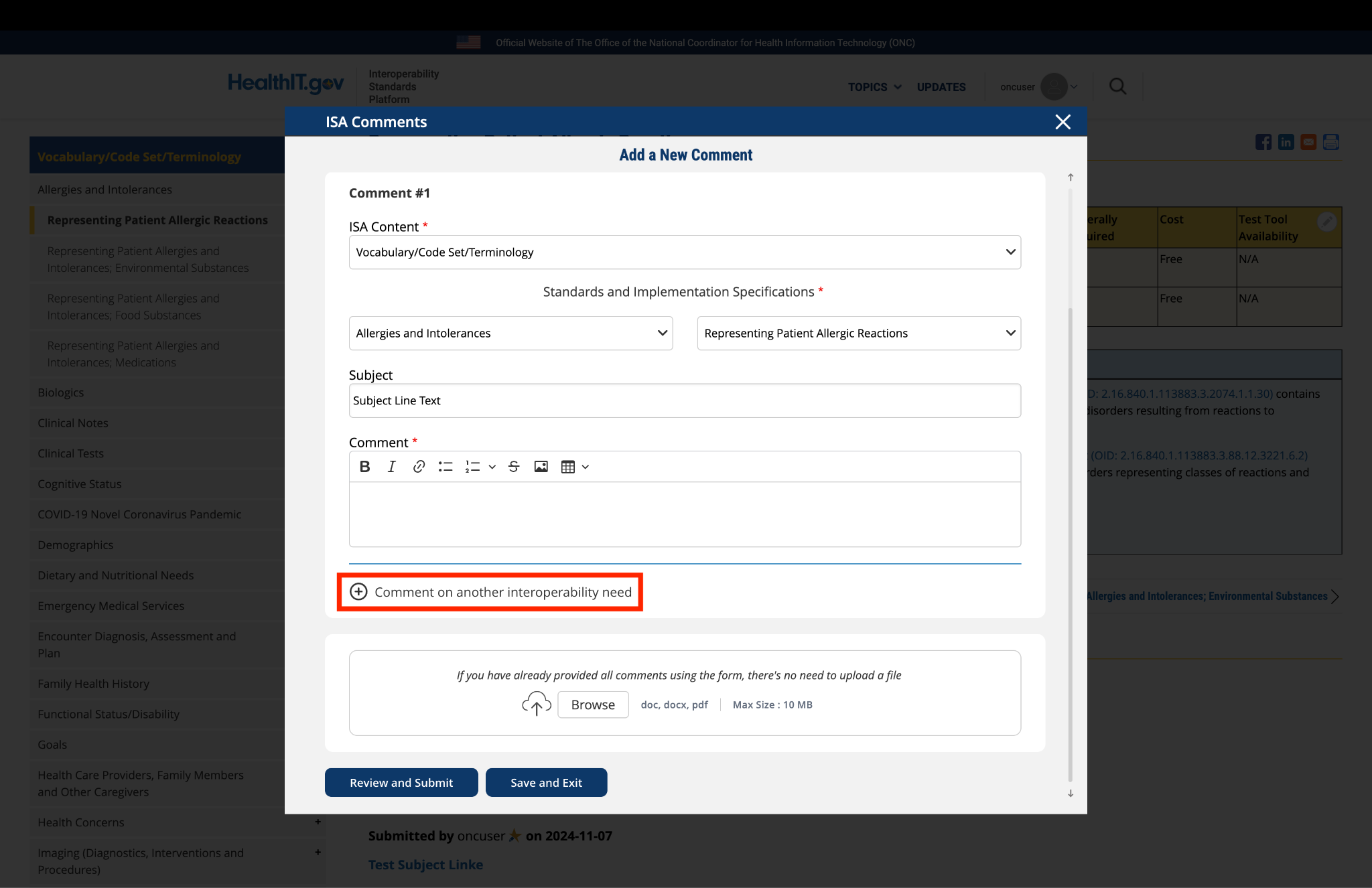
Fig 3 The "Comment on another interoperability need" link enables users to add multiple comments within a single submission.
4. Optional: Upload Supporting Files
The platform allows you to upload supporting documentation to enhance your comment:
- Locate the "File Upload" section at the bottom of the comment form.
- Click to upload any files (such as PDFs or documents) that provide additional context, evidence, or clarification for your comment.
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
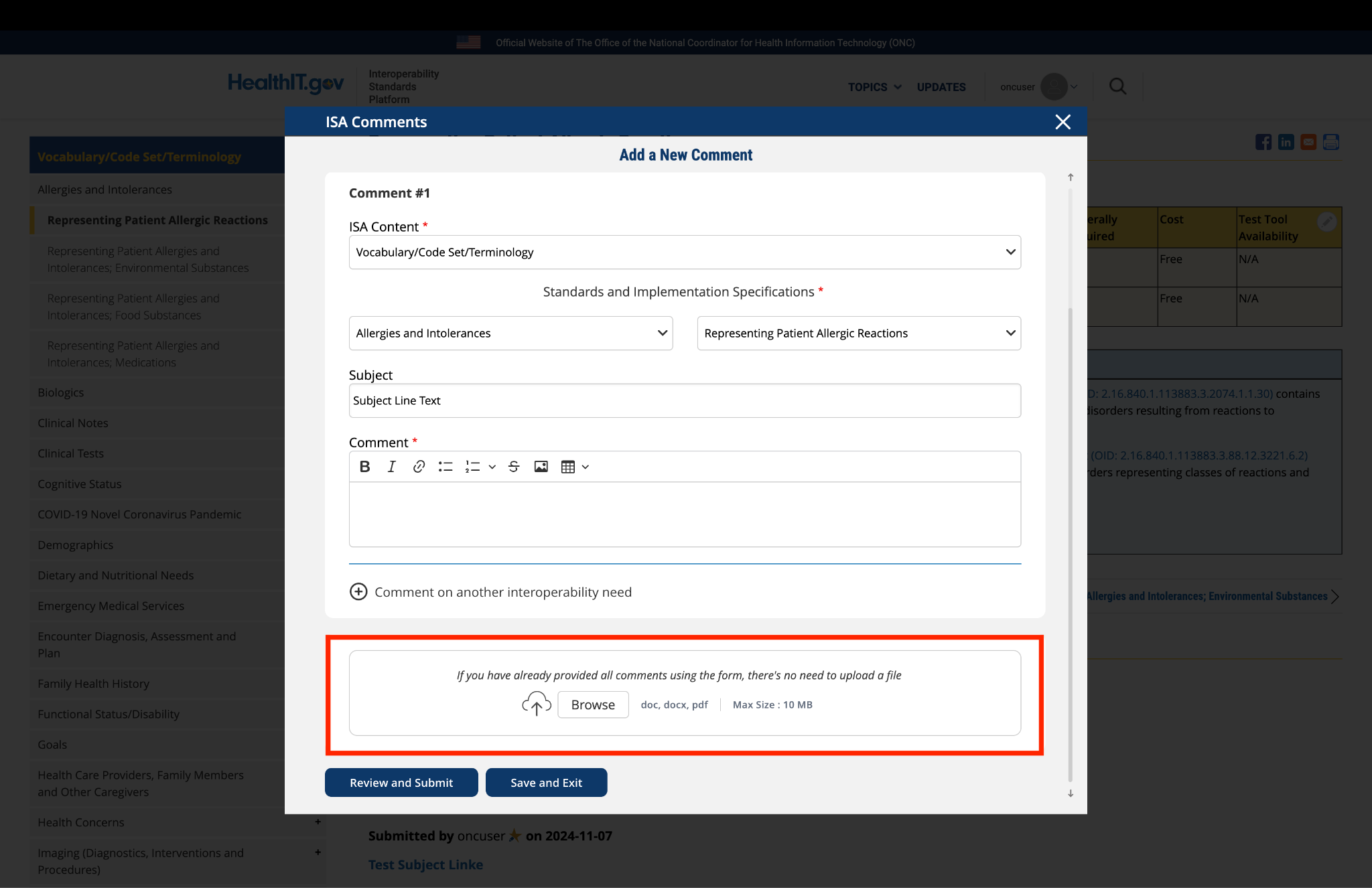
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
5. Optional: Save and Exit
If you need to pause your work and return to complete your comment later:
- Click the "Save and Exit" button at the bottom of the form.
- Your comment will be saved as a draft that you can access and complete later.
- When you return to the platform, you will see a red triangle with an exclamation mark next to the "Return to saved Comment" button, indicating that you have saved comments in draft status.
- Click the "Return to saved Comment " button to continue working on your draft.
- You will be taken to a review page where you can:
- Select "Submit Comment" to officially submit your feedback.
- Click "Edit" to return to the comment form and make changes
- Select "Discard Draft" to delete the saved draft and start fresh
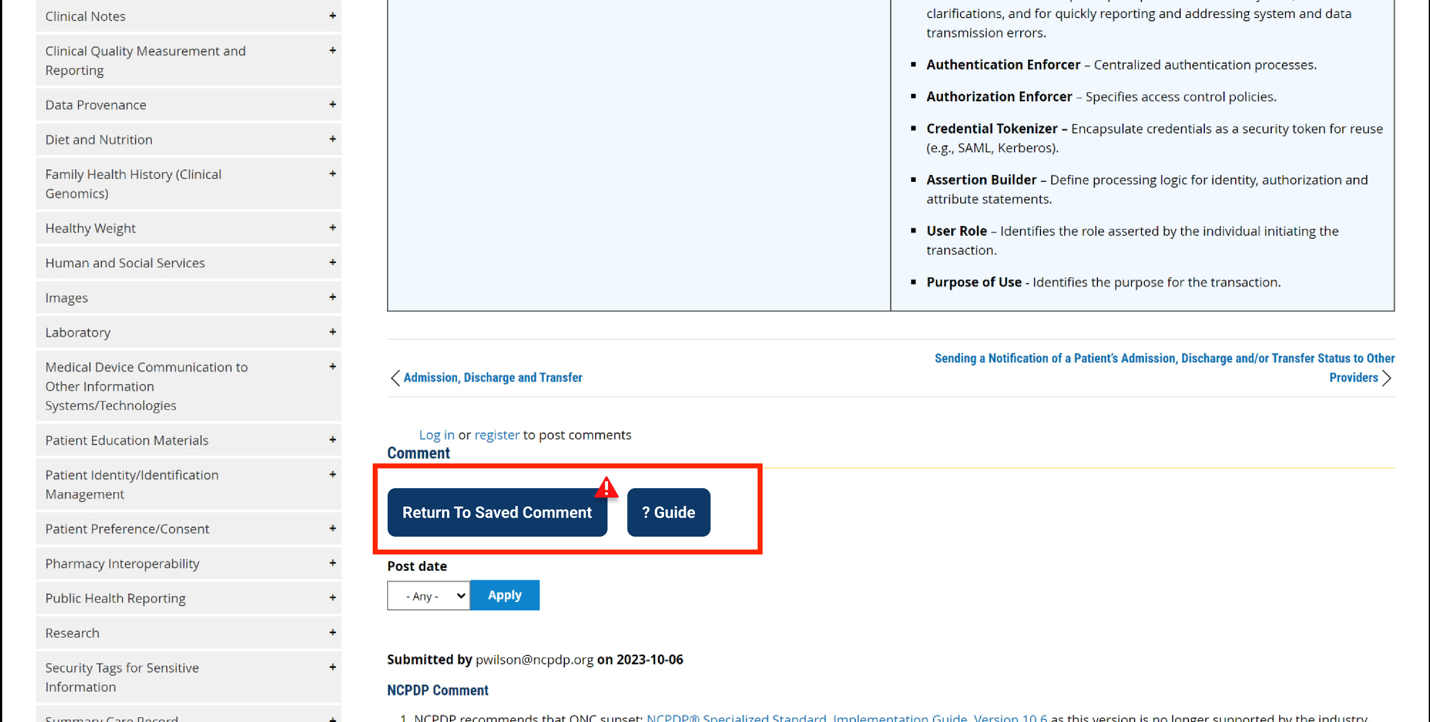
Fig 5 A red triangle with exclamation mark indicator appears next to the "Return to saved Comment" button when draft comments are saved in the system.
6. Review and Submit
Once you have completed your comment:
- Click the "Review and Submit" button at the bottom of the form.
- This will take you to a review screen displaying your comment(s) in full.
- Review all information for accuracy and completeness.
- On this review screen, you have three options:
- Click "Submit Comment" to officially submit your feedback
- Click "Edit" to return to the comment form and make changes
- Click "Discard Draft" to delete the comment and start fresh
- The review screen also includes a "Print" button that allows you to create a printed copy of your comments for your records.
- If you choose to submit, your comment will be recorded in the system and made available for review by the appropriate stakeholders.
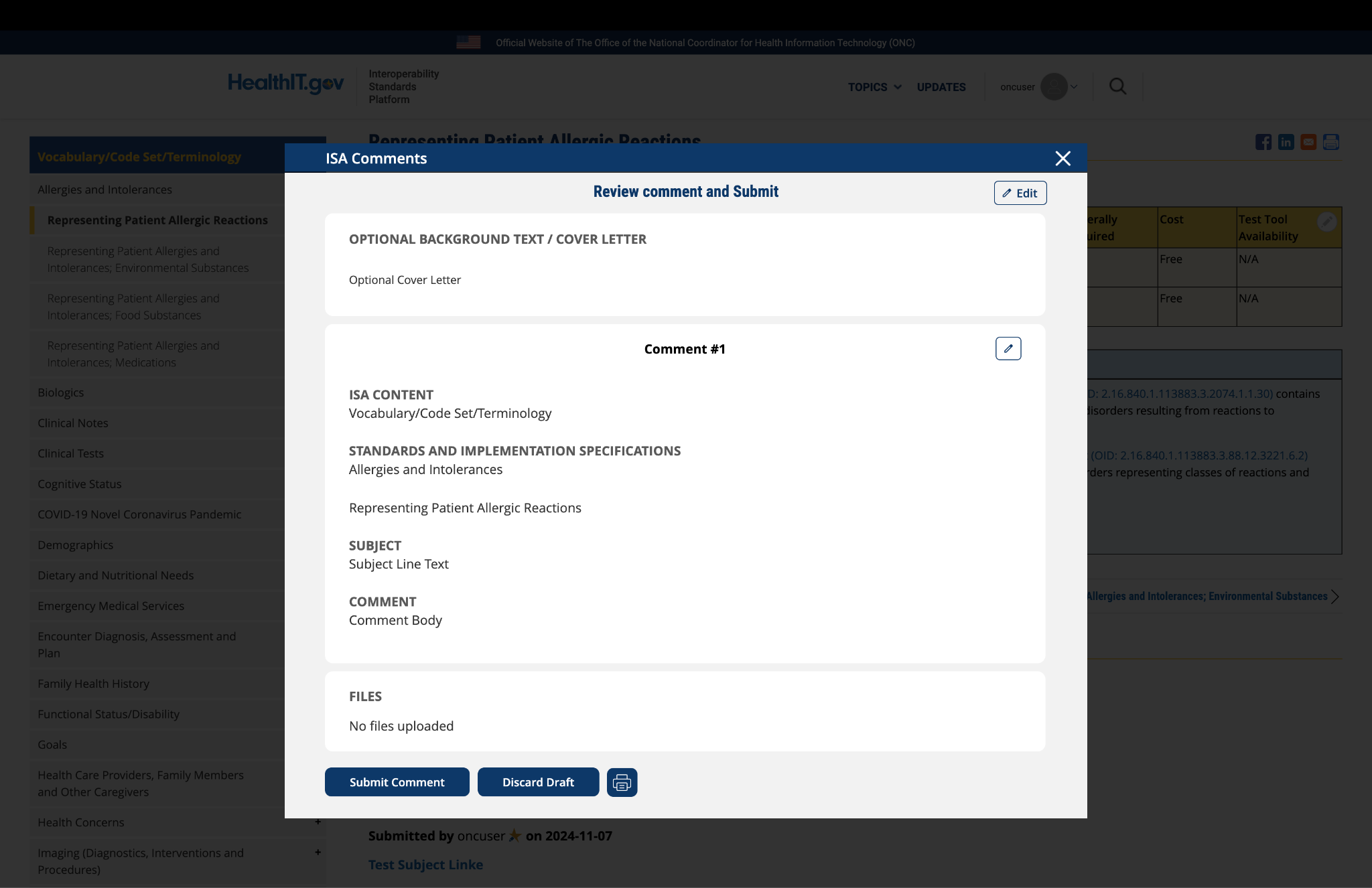
Fig 6 The review screen includes a "Print" button that allows users to create a record of their comment submission.
Comment
Submitted by reinaldovel on
Register for course Understanding Emerging API-Based Standards
How do I register for this course: Understanding Emerging API-Based Standards
Submitted by Brett Andriesen ![]() on
on
This is not a course, just…
This is not a course, just an educational description of API standards.
Submitted by mattreid on
Patient Privacy
The AMA wholeheartedly supports the right of patients to receive their medical information using smartphone applications (apps), but is concerned about the lack of safeguards to ensure that patients understand what they are consenting to when they grant permission to an app to access their information. These apps share sensitive health information with third parties, often without an individual's knowledge. Much of this information can end up in the hands of data brokers and be used or sold for advertising and marketing. Data being used in this way may ultimately erode patients’ privacy and their willingness to disclose information to their physicians.
As a first step to address this issue, the AMA is calling for controls to be instituted that establish transparency as to how health information is being used, who is using it, and how to prevent the profiteering of patients’ data. To help provide a minimal amount of transparency to patients about how a health app will use their health information, the federal movement should implement a basic privacy framework requiring certified EHR vendor APIs to check an app’s “yes/no” attestations to:
- Industry-recognized development guidance
- Transparency statements and best practices
- A clear privacy notice to patients
Submitted by pwilson@ncpdp.org on
NCPDP Comments
For details, refer to the Connectivity Operating Rules Implementation Guide at NCPDP Standards .