
| Type | Standard / Implementation Specification | Standards Process Maturity | Implementation Maturity | Adoption Level | Federally required | Cost | Test Tool Availability |
|---|---|---|---|---|---|---|---|
|
Standard
|
Final
|
Production
|
Yes
|
Free
|
N/A
|
| Limitations, Dependencies, and Preconditions for Consideration |
Applicable Value Set(s) and Starter Set(s)
|
|---|---|
|
Diagnosis and Conditions:
For genomic data:
For family relationships and roles:
|
Help
1. Optional: Background Text / Cover Letter
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
This field is entirely optional and serves the following purposes:
- Provides context for reviewers
- Serves as an introduction if submitting multiple comments
- Functions as a cover letter for formal submissions
If you are submitting a single comment for a specific data class or element, you may leave this field blank. For multiple comments, this space is useful for explaining the overall purpose or connection between your comments.
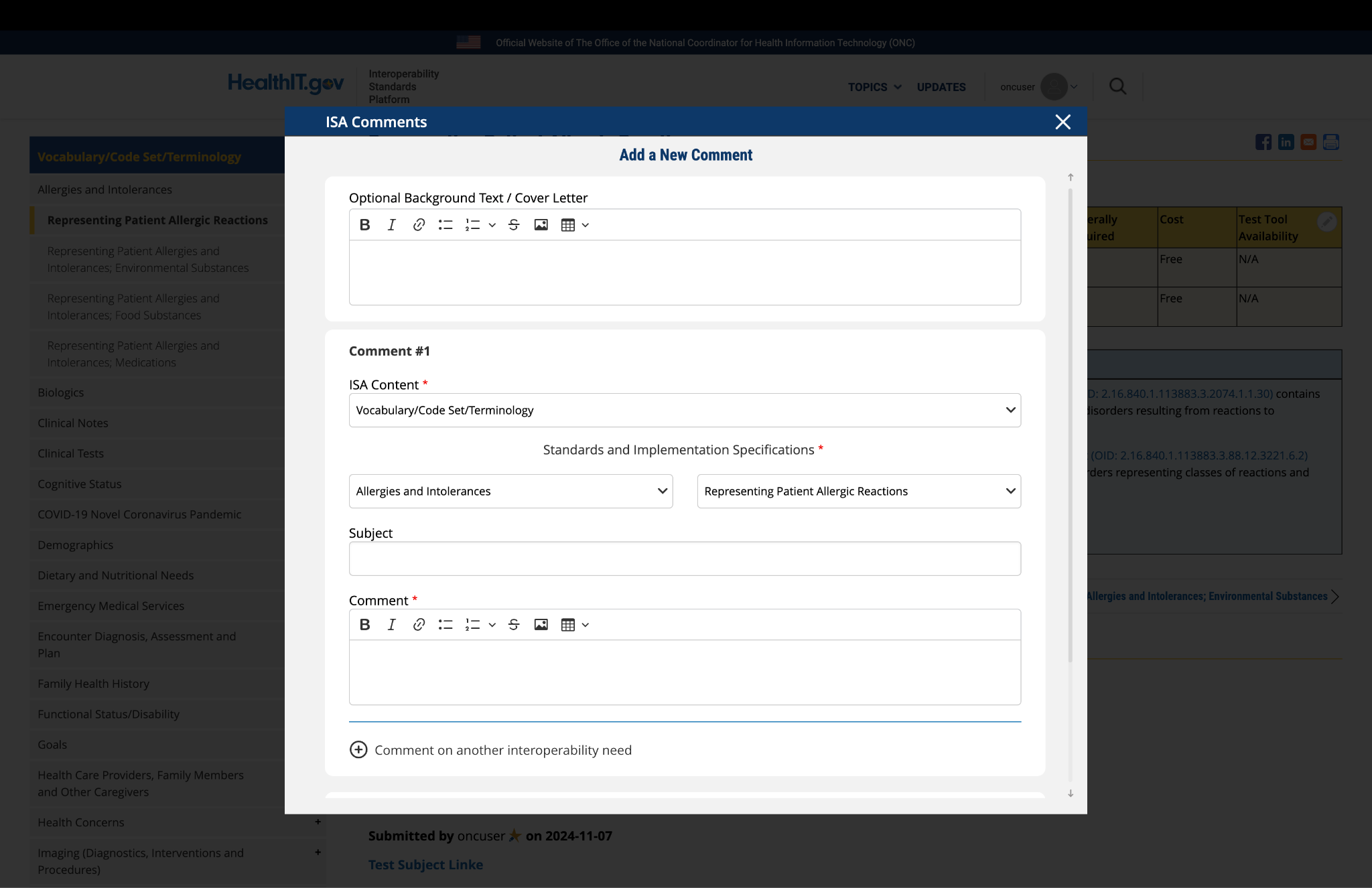
Fig 1 The "Optional Background Text / Cover Letter" field allows users to provide contextual information or introductory remarks for their comment submission.
2. Complete the Comment Form
The comment form contains several fields that require your input:
ISA Content: This field is automatically populated based on the page you are currently viewing. No action is required.
Standards and Implementation Specifications: This drop-down menu is pre-selected based on the topic you're commenting on. The selection reflects the relevant standard or implementation specification for your current page.
Subject: Enter a concise title that summarizes the focus of your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: This is the main field where you provide your detailed feedback, concerns, or suggestions. The comment box includes a text editor with formatting options that allow you to:
- Format text as bold or italic
- Insert hyperlinks
- Create bullet points
- Create numbered lists
- Apply strike-through formatting
- Attach images
- Insert tables
Use these formatting options as needed to clearly present your information.

Fig 2 The comment text editor toolbar provides formatting options including bold, italic, links, lists, tables, and image insertion capabilities.
3. Optional: Add Additional Comments
If you need to provide feedback on multiple aspects of the ISA content, you can add additional comments:
- After completing your first comment, locate and click the link labeled "Comment on another interoperability need" at the bottom of the form.
- A new comment section will appear, allowing you to enter details for your additional comment.
- For this new comment section, the "ISA Content" and "Standards and Implementation Specifications" fields will not be automatically populated. You must select the appropriate content and specification from the drop-down menus for each additional comment.
- Complete all required fields for your additional comment.
- Repeat this process for each additional comment you wish to submit.
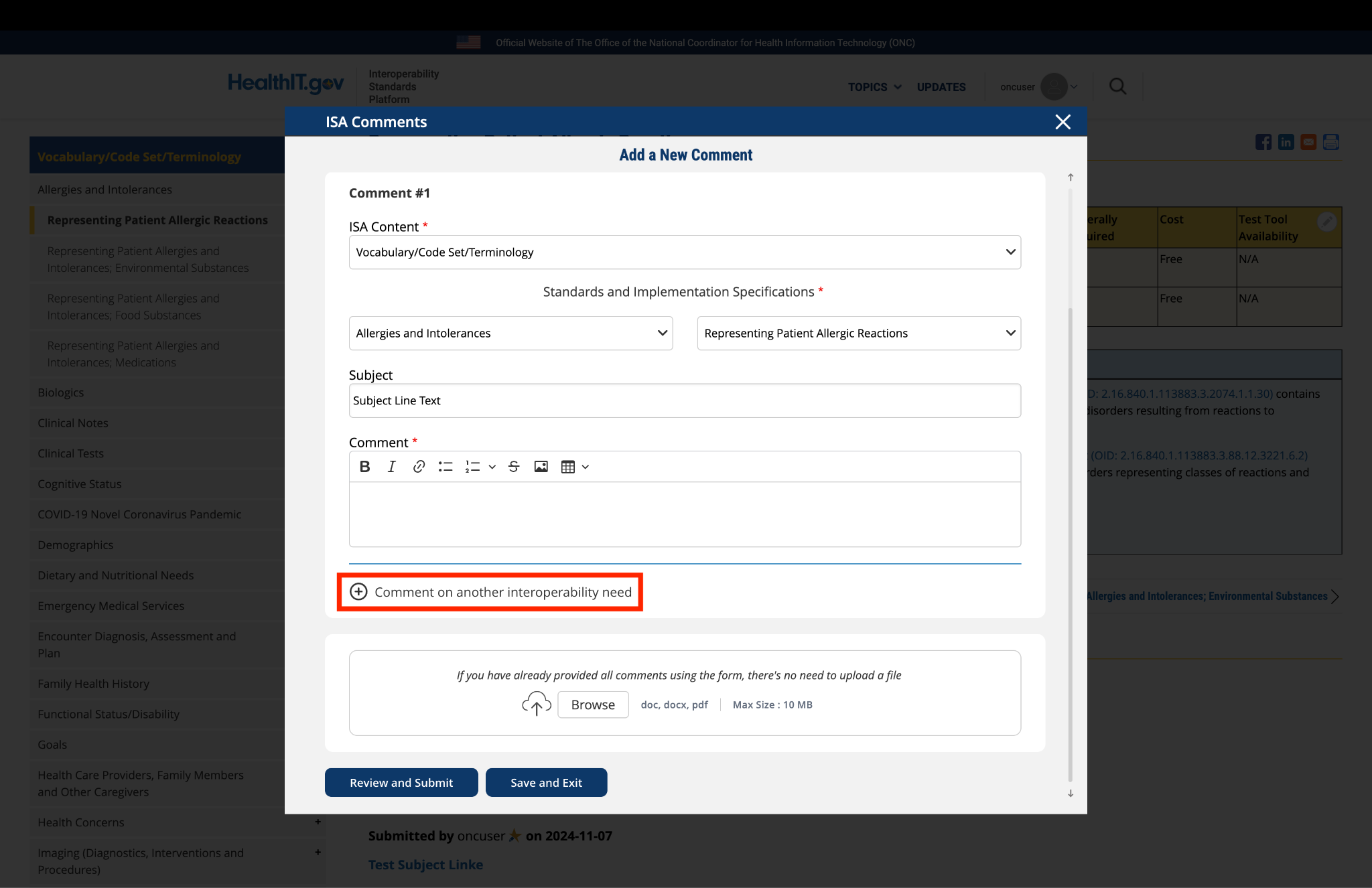
Fig 3 The "Comment on another interoperability need" link enables users to add multiple comments within a single submission.
4. Optional: Upload Supporting Files
The platform allows you to upload supporting documentation to enhance your comment:
- Locate the "File Upload" section at the bottom of the comment form.
- Click to upload any files (such as PDFs or documents) that provide additional context, evidence, or clarification for your comment.
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
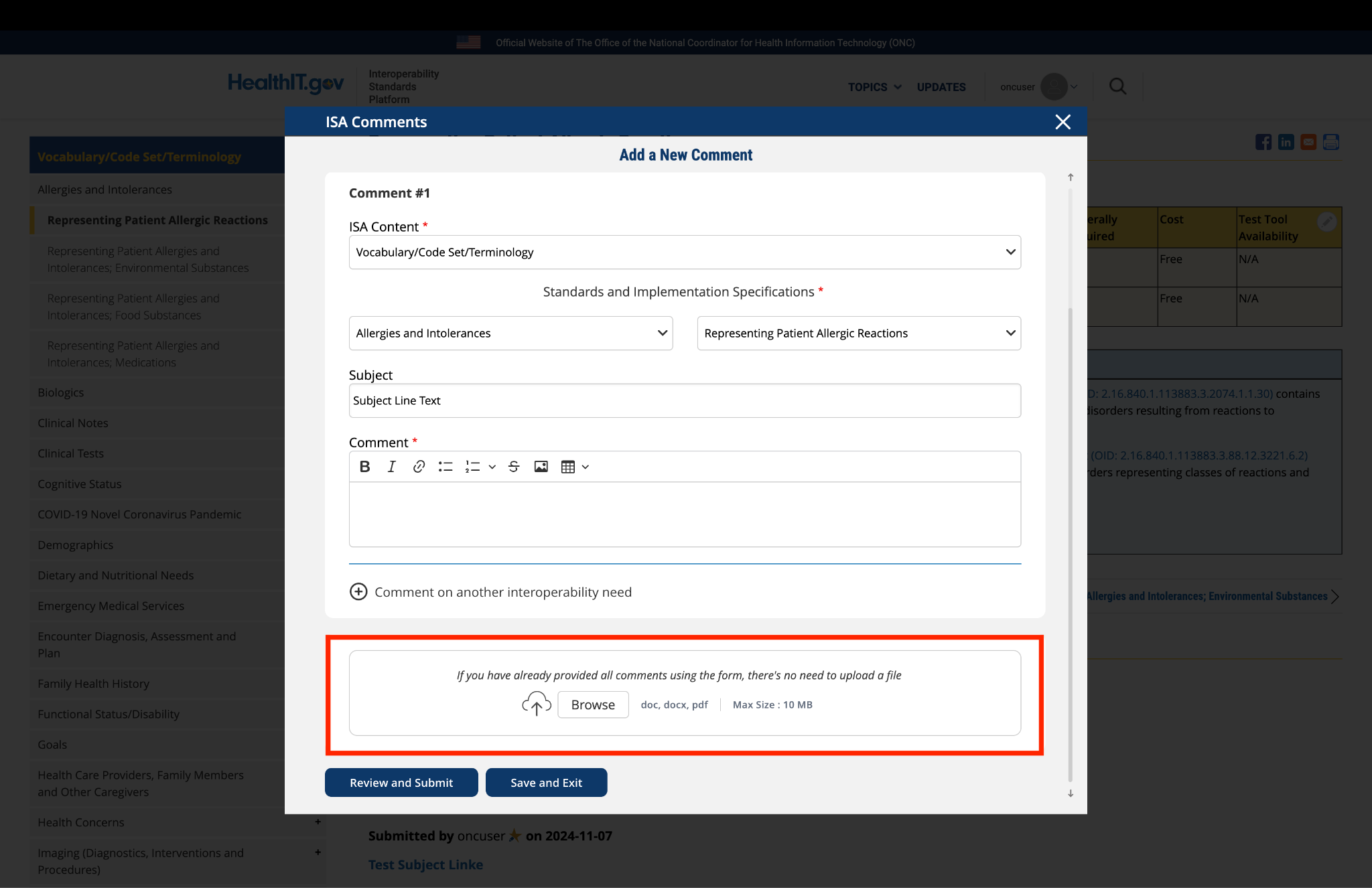
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
5. Optional: Save and Exit
If you need to pause your work and return to complete your comment later:
- Click the "Save and Exit" button at the bottom of the form.
- Your comment will be saved as a draft that you can access and complete later.
- When you return to the platform, you will see a red triangle with an exclamation mark next to the "Return to saved Comment" button, indicating that you have saved comments in draft status.
- Click the "Return to saved Comment " button to continue working on your draft.
- You will be taken to a review page where you can:
- Select "Submit Comment" to officially submit your feedback.
- Click "Edit" to return to the comment form and make changes
- Select "Discard Draft" to delete the saved draft and start fresh
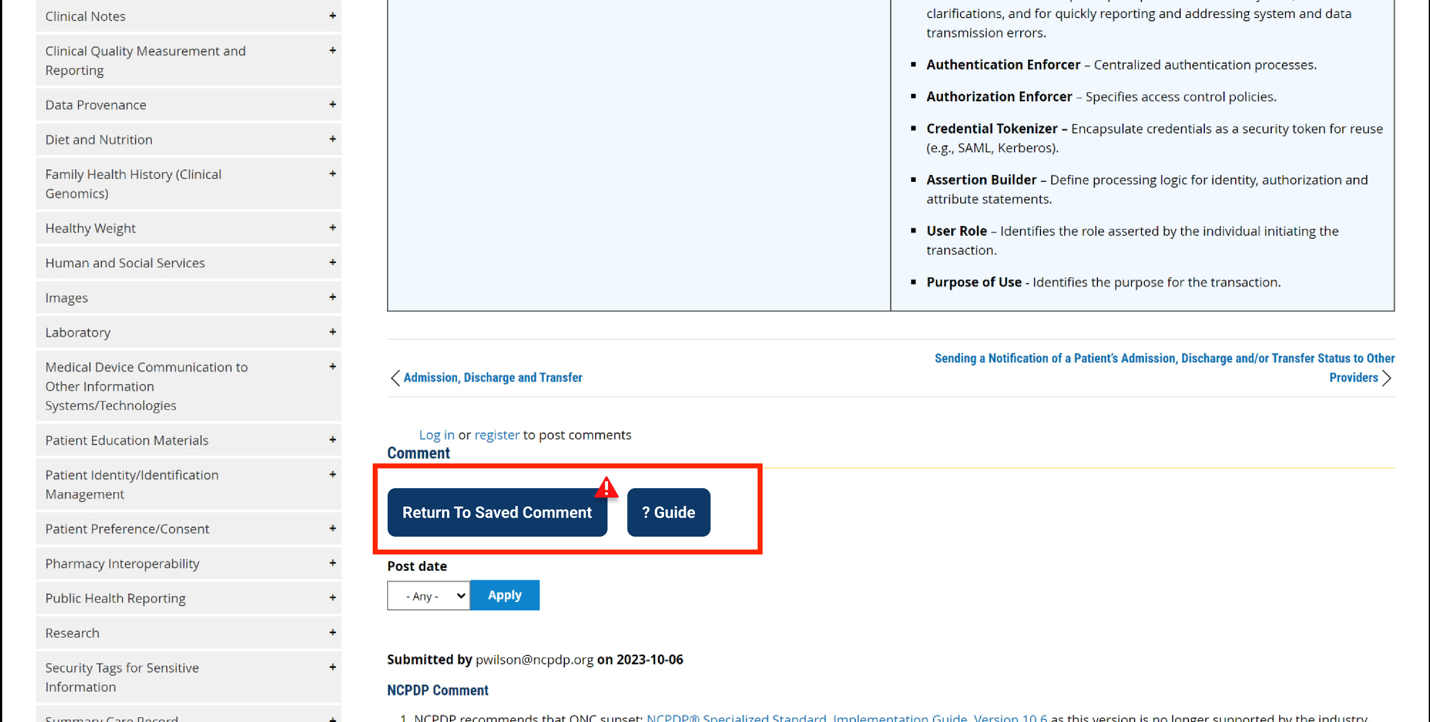
Fig 5 A red triangle with exclamation mark indicator appears next to the "Return to saved Comment" button when draft comments are saved in the system.
6. Review and Submit
Once you have completed your comment:
- Click the "Review and Submit" button at the bottom of the form.
- This will take you to a review screen displaying your comment(s) in full.
- Review all information for accuracy and completeness.
- On this review screen, you have three options:
- Click "Submit Comment" to officially submit your feedback
- Click "Edit" to return to the comment form and make changes
- Click "Discard Draft" to delete the comment and start fresh
- The review screen also includes a "Print" button that allows you to create a printed copy of your comments for your records.
- If you choose to submit, your comment will be recorded in the system and made available for review by the appropriate stakeholders.
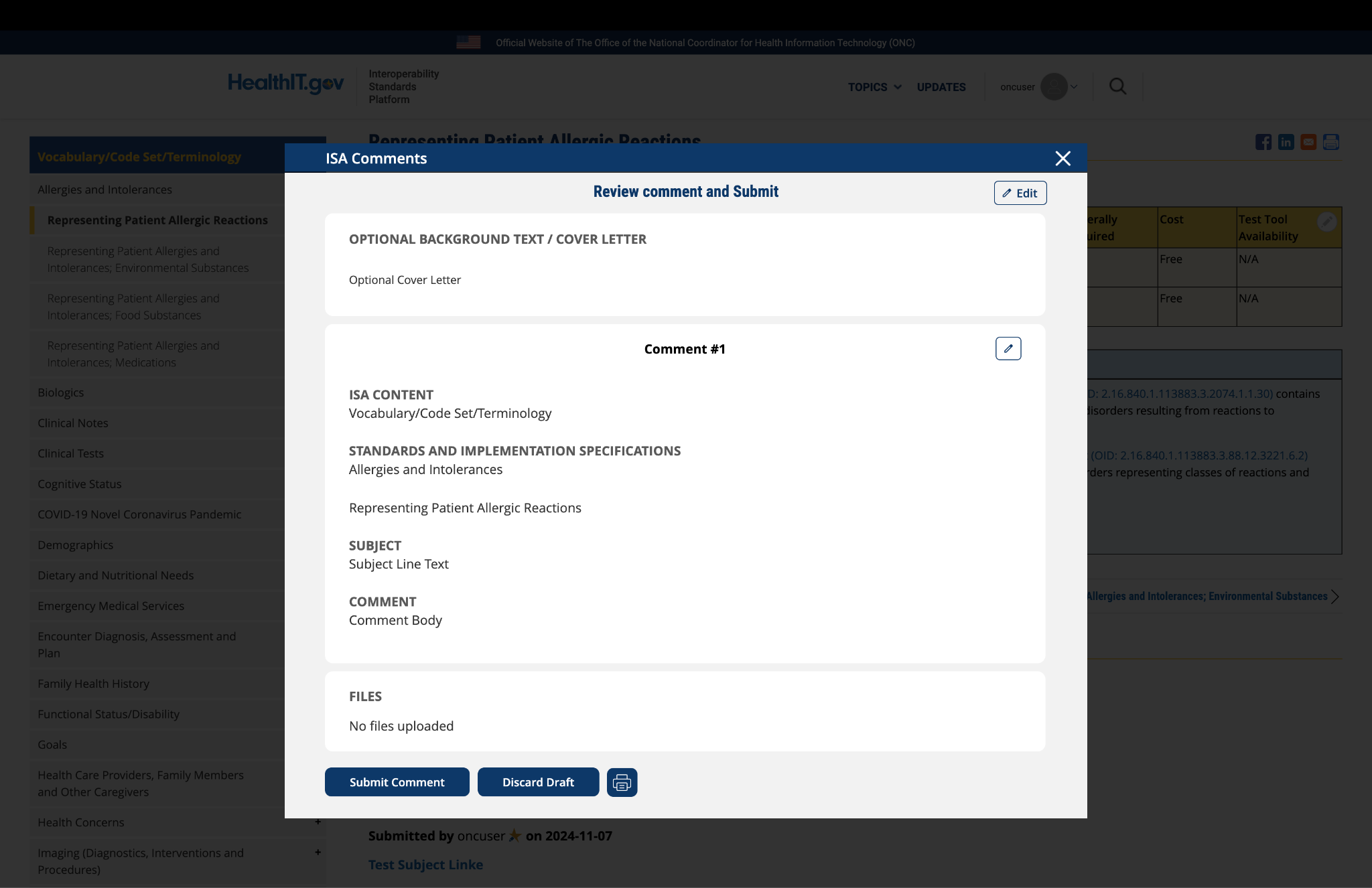
Fig 6 The review screen includes a "Print" button that allows users to create a record of their comment submission.
Comment
Submitted by mattreid on
The AMA requests that the…
The AMA requests that the Current Procedural Terminology (CPT) code set be added to the standards listed in Section I: Representing Patient Family Health History. The CPT Evaluation and Management codes specifically address capturing the patient’s family health history. The E/M codes specifically provide information about:
- The health status or cause of death of parents, siblings, and children;
- Specific diseases related to problems identified in the chief complaint or history of the present illness, and/or system review
- Diseases of family members that may be hereditary or place the patient at risk
Also, CPT code 96040 identifies medical genetics and genetic counseling services.
CPT is a comprehensive and regularly curated uniform language that accurately describes medical, surgical, and diagnostic services and provides for reliable communication among users. It has an extremely robust and mature development process with open and transparent meetings and clinical input from national medical specialties and relevant stakeholders. It is the most widely adopted outpatient procedure code set. Use of the CPT code set is federally required under HIPAA.
Submitted by ssvaby on
Wrong code system referenced for Problem Type
2.16.840.1.113883.3.88.12.3221.7.2 - this code system is not LOINC as referenced above...it is SNOMED.
Submitted by vojtech_huser on
feedback
Consider adding the following info to starter set
OMOP common data model is using SNOMED CT concepts (descendants of SNOMED CT term 125677006 (http://snomed.info/id/125677006)) to standardize family relationships (reference: https://github.com/OHDSI/CommonDataModel/wiki/FACT_RELATIONSHIP#conventions ).
Submitted by cmcdonald on
Standard for observation…
Standard for observation values: should probably be Standard for observation values that are represented as codes (won't apply if they are free text or numbers).
Many of the details of Family Genomic History are not capturable by SNOMED CT. They will require the code systems provided by NCBI such as ClinVar, dbSNP, etc.
This is a greatly exaggerated assessment in the CMS Assessments. A large provider of IHE interfaces see SNOMED CT codes for 5% or fewer variables with multiple choice answers. Most are either text and/or local codes.
Submitted by gdixon on
Are the value sets in ISA accounting for the decisions and imple
- Personal Relationship Role Type” Personal Relationship Role Type urn:oid:2.16.840.1.113883.1.11.19563
- There is a discrepancy between this value set and FHIR 4.0. More generally are the value sets in ISA accounting for the decisions and implementations being made with FHIR?
- Definition:
- A relationship between two people characterizing their "familial" relationship
- OID: 2.16.840.1.113883.1.11.19579 (for OID based terminology systems)
- Title: V3 Value SetFamilyMember
- Name: v3.FamilyMember
- Defining URL: http://terminology.hl7.org/ValueSet/v3-FamilyMember
- Definition:
Submitted by mcpatric on
NCBI genomic data resources
NCBI resources for sequences, including RefSeq, dbVar, and dbSNP, can be found here:
https://www.ncbi.nlm.nih.gov/guide/all/
Submitted by kwboone on
Need code system for family…
Need code system for family relationships, SNOMED CT and HL7 V3 Personal Relationship have good value sets for this.
Submitted by gldickinson on
Preserving Clinical Context
General Comments:
USCDI specifies lots of clinical data classes and data elements
It is crucial to consider and determine/resolve how clinical content and context are bound together and preserved in USCDI. The ultimate end user (often a clinician) must be able to readily discern context and inter-relationships – otherwise USCDI places an undue (and often unresolvable) burden on this user. Only the source EHR/HIT system can structure clinical content and context properly. Once data is stuffed into the USCDI framework and related exchange artifact (e.g., FHIR resources) this opportunity is forever lost.