Assessments of a health-related matter of interest, importance, or worry to a patient, patient’s family, or patient’s healthcare provider that could identify a need, problem, or condition.
Description (*Please confirm or update this field for the new USCDI version*)
Evaluation of a patient's current or usual exercise.
Examples include but are not limited to frequency of muscle-strengthening physical activity, days per week with moderate to strenuous physical activity, and minutes per day of moderate to strenuous physical activity.
Applicable Vocabulary Standard(s)
Applicable Standards (*Please confirm or update this field for the new USCDI version*)
Logical Observation Identifiers Names and Codes (LOINC®) version 2.77
Submitted By: Laurie P. Whitsel
/ American Heart Association/Physical Activity Alliance
Data Element Information
Rationale for Separate Consideration
Physical activity level, including aerobic activity and muscle strengthening, congruent with the Physical Activity Guidelines for Americans, are the foundation of the measures we are proposing to use. The measures we are proposing consists of two parts: the “Exercise Vital Sign” for aerobic activity and an assessment for muscle strengthening. However, these are not vital signs in the traditional sense and would not make sense to represent there, as they are an assessment of lifestyle, not of specific physiological measurements.
A low level of physical activity would often be a “Health Concern” and some systems may in fact track it this way. However, this proposed measure is much like Tobacco Use/Smoking in that it reflects “current state” of the patient, whether that is a cause for concern for intervention or not. As such, it makes sense to track physical activity level distinctly as a health concern and to create a Health Concern related to physical activity if necessary.
Use Case Description(s)
Use Case Description
Providers typically capture and share information about physical activity in the same manner as information about other lifestyle factors such as smoking and substance use. Clinicians assess a patient’s level of physical activity against the Physical Activity Guidelines for Americans based on age and may drive interventions such as counselling or referral.
Physical activity level can also be trended over time to help assess whether a patient’s levels are improving or declining.
Clinical systems share these measures as part of the referral process and as part of patient record transfers.
The Physical Activity Guidelines for Americans call for the capture of two measures – minutes/week of moderate to vigorous aerobic physical activity and days per week of muscle-strengthening activity. This proposal follows the literature-validated approach of splitting the first measure into two components of days/week and minutes/day, which patients have an easier time estimating and therefore produces a value more reflective of their actual aerobic activity level.
Device data, such as step counts and heart rate information, can sometimes support Exercise Vital Sign measures where patients have access to devices. However, further research and validation are necessary to integrate those kinds of measurements into assessment, prescription, referral and patient follow-through.
The page at the link below provides more detailed support for the importance of capturing and sharing physical activity information, including literature references.
Estimate the breadth of applicability of the use case(s) for this data element
Per the US Physical Activity Guidelines, practitioners should capture and assess this element for all patients beginning at the age of 3 years. This equates to hundreds of millions of patients and about a million physicians, nurses, and other clinicians.
Public health, payers, clinicians, and others have a significant interest in assessing the level of aerobic and muscle-strengthening physical activity across patient populations, given the correlation between physical activity levels and patient health outcomes. Systems may report physical activity levels as patient health measures or as part of public health surveillance on an identified or de-identified basis. This type of reporting is not currently common standard of practice but is growing to inform the relationship between physical activity and patient outcomes and improve physical activity public health surveillance across the US population.
When clinicians have identified a deficiency in a patient’s physical activity level, the clinician may refer the patient to the appropriate professional for interventions to help improve or sustain their physical activity levels. In such cases, clinical systems may communicate the physical activity measures to payers to support reimbursement for services and to service providers to provide an initial baseline for evaluation. Patients may also regularly capture the measures and share them with ordering providers, service providers, and-or payers to monitor progress.
Estimate the breadth of applicability of the use case(s) for this data element
Approximately 75% of the U.S. population is inactive or otherwise do not meet the Physical Activity Guidelines. This includes about 75% of school-age children (83% of adolescents) who do not meet the recommended levels of physical activity. For adults 65 years and older, more than 86% do not meet the Guidelines. While not all would qualify for intervention, it is important to move toward standardizing exchange of this data element across health systems, payers, service providers and public health surveillance to optimize patient health outcomes.
Maturity of Use and Technical Specifications for Data Element
Applicable Standard(s)
The following LOINC codes correspond to components of the proposed measures:
89555-7 – Physical Activity – Days/Week
68516-4 – Physical Activity – Minutes/Day
82291-6 – Physical Activity – Muscle-Strengthening
For the overall minutes/week measure, there is a standard LOINC code 89574-8 – Exercise Vital Sign that groups the Days/Week and Minutes/Day component, however it does not actually support capturing the calculated Minutes/Week component, even though the submitter of the code (Kaiser Permanente) makes regular use of the calculated value. HL7 will work with Kaiser and Regenstrief to either allow the existing ‘panel’ code to capture the calculated days/week measure or add an additional component that supports the calculation, making it easier to query for patients outside guideline without requiring client-side calculation.
The Physical Activity FHIR implementation guide is going to ballot in the 2023-May cycle and HL7 should published it in Fall, 2023. HL7 hosts the draft continuous integration build version here: https://build.fhir.org/ig/HL7/physical-activity.
Current Use
In limited use in production environments
Supporting Artifacts
The two components of the Exercise Vital Sign are part of the 2015 Certification Companion Guide on Social, psychological, and behavioral data (Paragraph (a)(15)(v)). A sizable portion of the U.S. EHR population has voluntarily certified to these criteria.
Of the few healthcare systems that collect physical activity data, Kaiser Permanente is the largest system. Kaiser Permanente insures over 12 million people. Utilizing the Exercise Vital Sign, it is asked at every outpatient encounter with a healthcare provider. During 2020, there were over 31 million scheduled visits, which suggests this measure is quite extensively used each year.
5 or more. This data element has been tested at scale between multiple different production environments to support the majority of anticipated stakeholders.
Supporting Artifacts
There are about 150 EHR systems that have met the certification criteria for §170.315(a)(15) Social, Psychological, and Behavioral Data. This represents about 30% of the commercially available EHR systems voluntarily including this into their systems, suggesting a significant interest in the wider adoption of this standard. These criteria include two questions regarding physical activity like what we are proposing.
If we consider the use of the Exercise Vital Sign we propose, in the Kaiser Permanente system, the Exercise Vital Sign is asked at every care visit in their network of over 700 medical offices and other healthcare facilities. That represents extensive use of exchanging data between the various healthcare facilities, as well as to patients.
Other healthcare systems, such as Intermountain Health, use the Physical Activity Vital Sign (a similar questionnaire as the Exercise Vital Sign) within their EHR at their 225 medical offices. Furthermore, Prisma Health in Greenville, SC has twenty medical offices that participate in a physical activity assessment and referral program, Exercise is Medicine – Greenville. Staff screen participants for physical activity using the Physical Activity Vital Sign recorded into the EHR system. Their systems exchange the information with local YMCA organizations and patients. These are just examples of health systems where organization are integrating the data element into their standard of care.
Restrictions on Standardization (e.g. proprietary code)
The base components of the measure are all freely available LOINC codes and we do not anticipate an issue in either updating an existing LOINC code or introducing a new one to capture the total minutes/week measure.
There are other measures that are used in parts of healthcare to assess physical activity, including the Rapid Assessment of Physical Activity and Physical Activity Vital Sign which were reviewed in a 2018 AHA Scientific Statement . However, based on a literature scan as well as an HL7-convened expert group, it seems that the Exercise Vital Sign is the most appropriate and widely used measure and is an appropriate foundation to drive increased standardization.
Restrictions on Use (e.g. licensing, user fees)
None
Privacy and Security Concerns
This information could fall under the banner of personally identifiable healthcare information under HIPAA if captured in a healthcare setting, though it has a lower sensitivity level than most healthcare data. If captured and shared outside of a healthcare setting (e.g., on a personal device or shared between a patient and a personal trainer), there would be no HIPAA restrictions.
Estimate of Overall Burden
Nearly all patients can estimate these values and the effort should require minimal time (~30 seconds) to report either by questionnaire or in conversation with a practitioner. Clinicians would typically gather this information as part of the same workflow as other lifestyle measures such as smoking and substance use. Where a patient engages in ongoing monitoring, it would typically only require reporting one measurement per month.
At present, devices are providing supporting data such as heart rates, step counts, move minutes, exercise modality, etc. However, there is opportunity for the device data reporting to be more precisely congruent with Physical Activity Guidelines recommendations.
EHR implementation would build on existing support for reading and writing Observation-based data and would fit into existing standards-based capture of lifestyle information. For those systems that already adhere to the optional certification criteria, it would only mean introducing the one new strength-based measure, which should fit into the same workflow, user-interface, and data exchange code.
Other Implementation Challenges
Because the patients report and estimate the values, accuracy can vary. However, high accuracy is not necessary. Precision within 20-30% is sufficient for determining whether intervention is necessary or appropriate. Eventually, device data may be an important supplement or affirmation of self-reported data.
This information is rarely culturally sensitive, though some patients may feel reluctant to share their information.
ASTP Evaluation Details Each submitted Data Element has been evaluated based on the following criteria. The overall Level classification is a composite of the maturity based on these individual criteria. This information can be used to identify areas that require additional work to raise the overall classification level and consideration for inclusion in future versions of USCDI
Criterion #1 Maturity - Current Standards
Level 2 - Data element is represented by a terminology standard or SDO-balloted technical specification or implementation guide.
Criterion #2 Maturity - Current Use
Level 2 - Data element is captured, stored, or accessed in multiple production EHRs or other HIT modules from more than one developer.
Criterion #3 Maturity - Current Exchange
Level 2 - Data element is electronically exchanged between more than two production EHRs or other HIT modules of different developers using available interoperability standards.
Criterion #4 Use Case(s) - Breadth of Applicability
Level 2 - Use cases apply to most care settings or specialties.
Please find attached Lakeshore's letter to express our support for the Physical Activity Alliance's application to add Physical Activity Status as a data element to the next iteration of the US. Core Data for Interoperability (USCDI).
Please find attached the National Athletic Trainers’ Association letter of support for the Physical Activity Alliance’s application to add Physical Activity Status as a data element to the next iteration of the U.S. Core Data for Interoperability (USCDI).
The concepts outlined under Physical Activity (e.g., days/week and hours/day of Physical Activity; and muscle strengthening) in the applicable vocabulary standards identify Logical Observation Identifiers Names and Codes (LOINC®) version 2.73. However, there are similar concepts that are in SNOMEDCT that may be in use (e.g., SCTID: 639700 - Muscular strength development exercise (regime/therapy)) that should be included. Suggest that the equivalent concepts in SNOMEDCT are supported.
IHRSA - The Global Health & Fitness Association supports the Physical Activity Alliance submission of the Physical Activity Status data element to standardize the assessment of physical activity (PA) into the U.S. Core Data for Interoperability (USCDI), including all four applicable standards addressing the components of aerobic and muscle strengthening PA. Please find the attached letter of support.
NCPDP supports the use of LOINC codes for assessments and observations for physical activity. NCPDP utilizes LOINC codes in the HL7/NCPDP Pharmacist eCare Plan.
I am writing to express my support for the Physical Activity Alliance's application to add Physical Activity Status as a data element to the next iteration of the US Core Data for Interoperability.
The proposed Physical Activity Status data element is comprised of four standardized measures:
(1) Average frequency of moderate to strenuous exercise each week;
(2) Average duration of moderate to strenuous exercise;
(3) Total minutes of moderate-vigorous physical activity/week; and
(4) Average frequency of muscle-strengthening exercise each week.
These measures are validated in the peer-reviewed literature1,2 and are aligned with the 2018 U.S. Physical Activity Guidelines for Americans.3
Integrating the Physical Activity Status data element into existing platforms is readily feasible for electronic health record systems. In fact, two of the measures are already included in the voluntary 2015 Certification Companion Guide on Social, Psychological, and Behavioral data (Paragraph (a)(15)(v)); which is currently followed by approximately 150 electronic health record systems in the U.S. Therefore, for the systems that already adhere to the certification criteria, adding the Physical Activity Status data element would simply require the introduction of the muscle-strengthening measure, which should fit into the existing workflow, user- interface, and data exchange codes. Furthermore, the Physical Activity Alliance is developing a HL7 FHIR implementation guide involving the proposed measures, which we expect will be sent to balloting in May 2023 and published in the Fall of 2023.
Being physically active is one of the most important lifestyle behaviors for maintaining physical health, mental health, and well-being.3 As a primary care sports medicine physician practicing musculoskeletal medicine daily, physical activity is a critical part of every conversation whether they are young or old and regardless of their current level of exercise and physical activity. In my two leadership roles, medical director of the Women's Sports Medicine Center and incoming President of the American Medical Society for Sports Medicine, I regularly advocate for many components of physical activity. Physical activity is included in our intake forms for all patients asking details related to the data elements above. Having this as a standard data element would enhance how practitioners across the nation discuss physical activity with their patients which is especially important now since so much is known of the value of physical activity yet we are in an epidemic of sedentary lifestyle.
Evidence suggests that routine assessment of physical activity by clinicians leads to more referrals for exercise programming, greater weight loss for patients with obesity, and improved hemoglobin A1c levels in patients with diabetes.4 Despite these potential outcomes, however, widespread implementation of physical activity assessment is inhibited by the lack of standardized physical activity measures. Adding Physical Activity Status to the USCDI would further solidify and standardize physical activity measures in the electronic health records in the U.S., which could dramatically improve the health of the public and bring U.S. healthcare costs down.5 Therefore, we urge ONC to maintain Physical Activity Status as a data element within the final USCDI version 4.
Thank you.
Sincerely,
Marci Goolsby, MD, FAMSSM
Primary Care Sports Medicine, Hospital for Special Surgery (HSS) New York, NY
Medical Director, Women's Sports Medicine Center at HSS
1st Vice President, American Medical Society for Sports Medicine
1 Coleman KJ, Ngor E, Reynolds K, Quinn VP, Koebnick C, Young DR, Sternfeld B, Sallis RE. Initial validation of an exercise “vital sign” in electronic medical records. Med Sci Sports Exerc. 2012;44:2071–2076. doi:10.1249/MSS.0b013e3182630ec1
2 Harris C, Watson K. A data users guide to the BRFSS physical activity questions: How to assess the 2008 Physical Activity
Guidelines for Americans. Atlanta, GA: CDC; 2011.
3 US Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd edition. 2018.
The Centers for Disease Control and Prevention supports adding physical activity to the USCDI. Physical activity is an important health behavior and like smoking and alcohol consumption should be included in routine clinical assessment. We support the addition of the Physical Activity Status Panel to the next version of the USCDI. In addition to voicing our support, we would like to reinforce the need to include all four data elements for physical activity required to meet/assess/measure compliance with national PA guidelines:
The frequency of aerobic activity in episodes per week,
The average usual duration of aerobic activity episodes,
A calculated value multiplying #1 and #2 to arrive at minutes per week, and
The number of episodes per week of muscle strengthening activity).
To obtain the full health benefits of physical activity, the Physical Activity Guidelines for Americans (2nd edition) (PAG) recommends, for example, that adults perform at least 150 minutes per week of at least moderate-intensity aerobic physical activity (the aerobic guideline) in addition to performing muscle strengthening activity that includes all major muscle groups at least twice weekly (the muscle-strengthening guideline). Other recommendations in the PAG also apply to young people and older adults. The peer-reviewed science that forms the basis of the Guidelines recommends this combination of activities because it is important for optimal health and thus, is important to monitor in the clinical setting. The four physical activity elements proposed to add to the USCDI are necessary to measure whether people are meeting these two guidelines
Comments from NACCHO: NACCHO supports the inclusion of the data element physical activity status. At the local health level, having this data will aid in creating community health assessments (i.e., chronic disease health assessments) and community health improvement plans.
This field is for general comments on this specific data element. To submit new USCDI data classes and/or data elements, please use the USCDI ONDEC system: https://healthit.gov/ONDEC
Please see the attached letter of support from the American College of Lifestyle Medicine for the Physical Activity Alliance's application to add to add Physical Activity Status as a data element to the next iteration of the U.S. Core Data for Interoperability (USCDI).
Comment submission on behalf of Dr. Michelle Albert, AHA President (2022-2023)
The American Heart Association (AHA) supports the addition of the draft data element to standardize the assessment of physical activity (PA) into the U.S. Core Data for Interoperability (USCDI), including all four applicable standards addressing the components of aerobic and muscle strengthening physical activity. The AHA has been supporting the “It’s Time to Move” initiative by helping to convene experts, work with regulatory agencies, engage in the HL7 process, and manage the HL7 project work group calls for developing the Physical Activity FHIR Implementation Guide. We encourage ONC to include the entire PA data element in the final version 4 of USCDI.
Please find attached The Coalition of the Registration of Exercise Professionals’ letter of support for the Physical Activity Alliance’s application to add Physical Activity Status as a data element to the next iteration of the U.S. Core Data for Interoperability (USCDI).
The "Optional Background Text / Cover Letter" field provides space for additional context or introductory information related to your comment.
If you wish to provide context, explanation, or an introduction to your comment, enter this information in the field labeled "Optional Background Text / Cover Letter." This is entirely optional and is most useful when submitting multiple related comments or when additional background would help reviewers understand your feedback.
If you are only commenting on a single data class or element, you may leave this field blank.
2. Select the Data Class
To specify which data class your comment addresses:
In the "Data Class" drop-down menu, select the appropriate data class you want to comment on.
If you are providing a general comment that is not specific to a data element, select "General" from the options. Comments with this designation will be displayed on the USCDI landing page.
Note that the Data Class field will automatically populate based on your current location in the platform:
If you are on a data class page, the field will be set to that specific data class
If you are on a data element page, the corresponding data class will be pre-selected
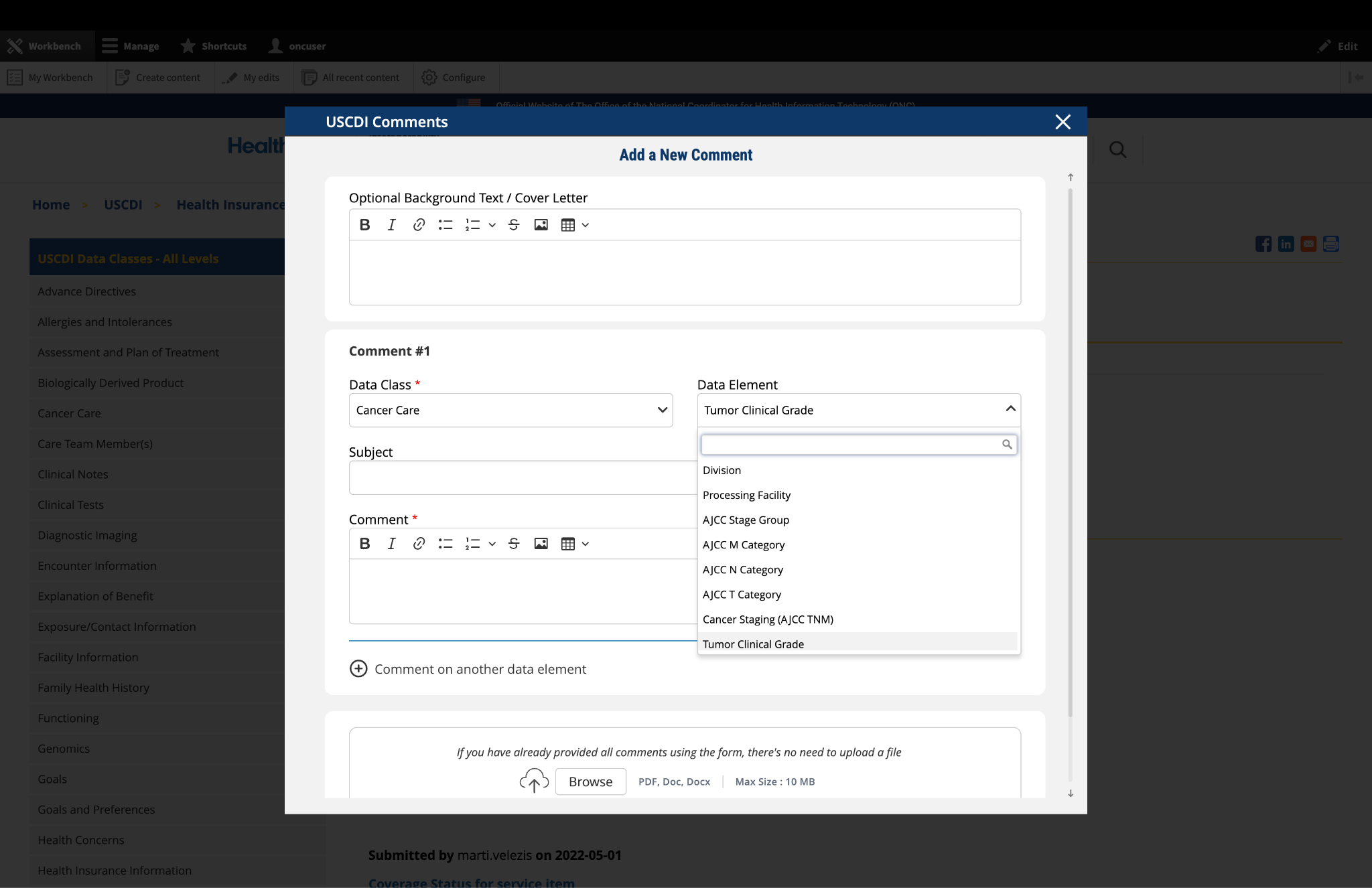
3. Select the Data Element
To specify which data element your comment addresses:
In the "Data Element" drop-down menu, select the specific data element you want to comment on.
The drop-down menu will display only the elements available under the data class you selected in the previous step.
You can use the search function within the drop-down to quickly locate a specific data element.
If you are commenting on the data class itself rather than a specific element, you may leave this field blank.
Note: Comments on a specific data element will appear on the respective data element page, while comments on a data class (without a specific element selected) will appear on the landing page for that data class.
Fig 1 The "Data Class" and "Data Element" dropdown menus allow users to specify the exact content they wish to comment on.
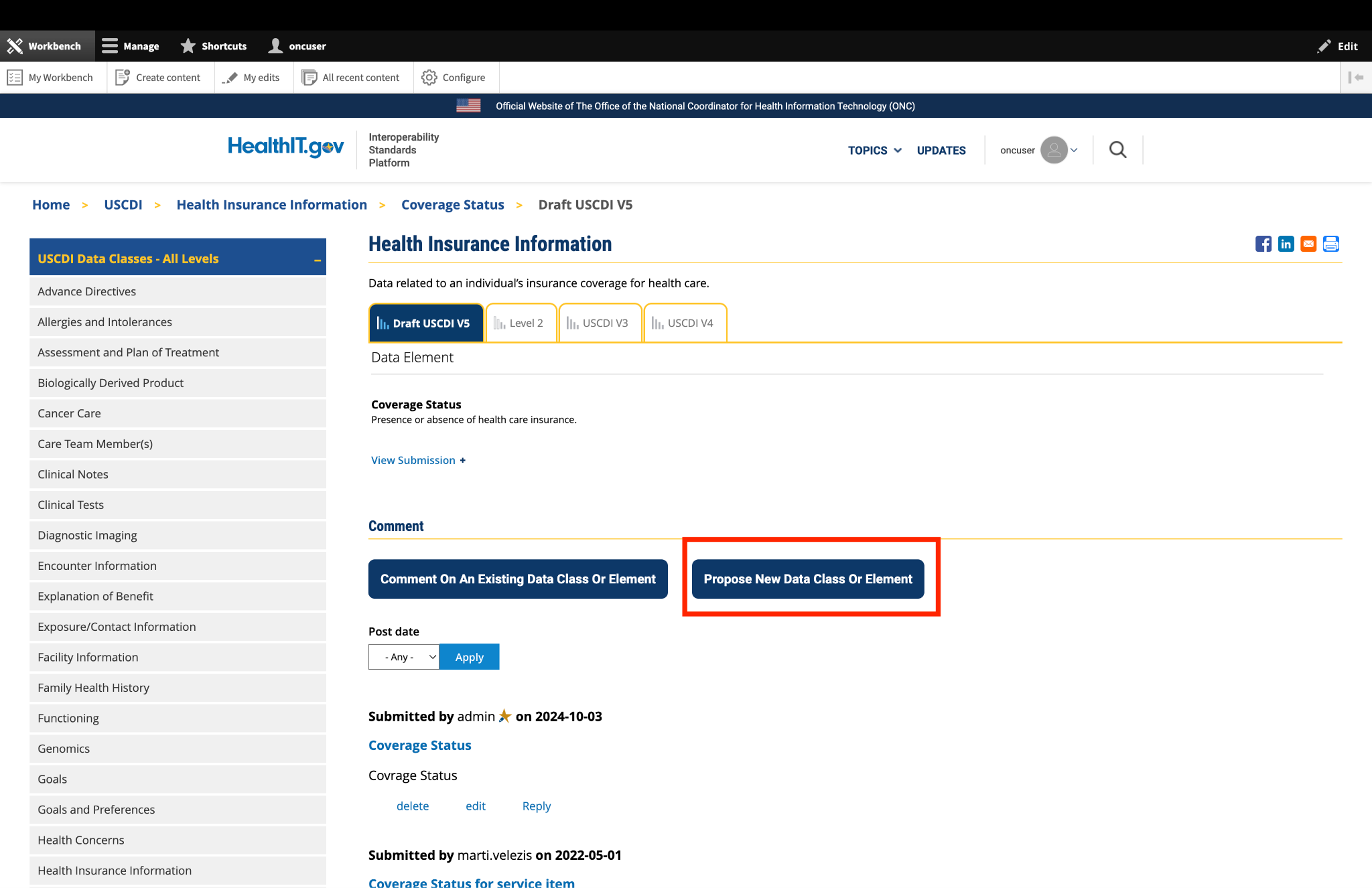
4. Optional: Propose New Data Class or Element
If you cannot find the appropriate data class or element for your comment:
Instead of clicking the "Comment On An Existing Data Class Or Element" button, click the adjacent button labeled "Propose a New Data Class or Data Element."
This will redirect you to the ONDEC (ONC New Data Element and Class) Submission System.
In the ONDEC system, follow the provided instructions to submit your proposal for a new data class or element.
Once your proposal is submitted through ONDEC, it will be reviewed separately from the commenting process.
Fig 2 The "Propose a New Data Class or Data Element" button redirects users to the ONDEC Submission System for proposing new data elements not currently available in the system.
5. Complete the Comment Form
Fill out the required fields in the comment form:
Subject: Enter a brief, descriptive title that summarizes your comment. This helps reviewers quickly understand the nature of your feedback.
Comment: In this field, provide the full details of your comment or feedback. Be as clear and specific as possible about your suggestions, concerns, or observations. Include any relevant details that support your position.
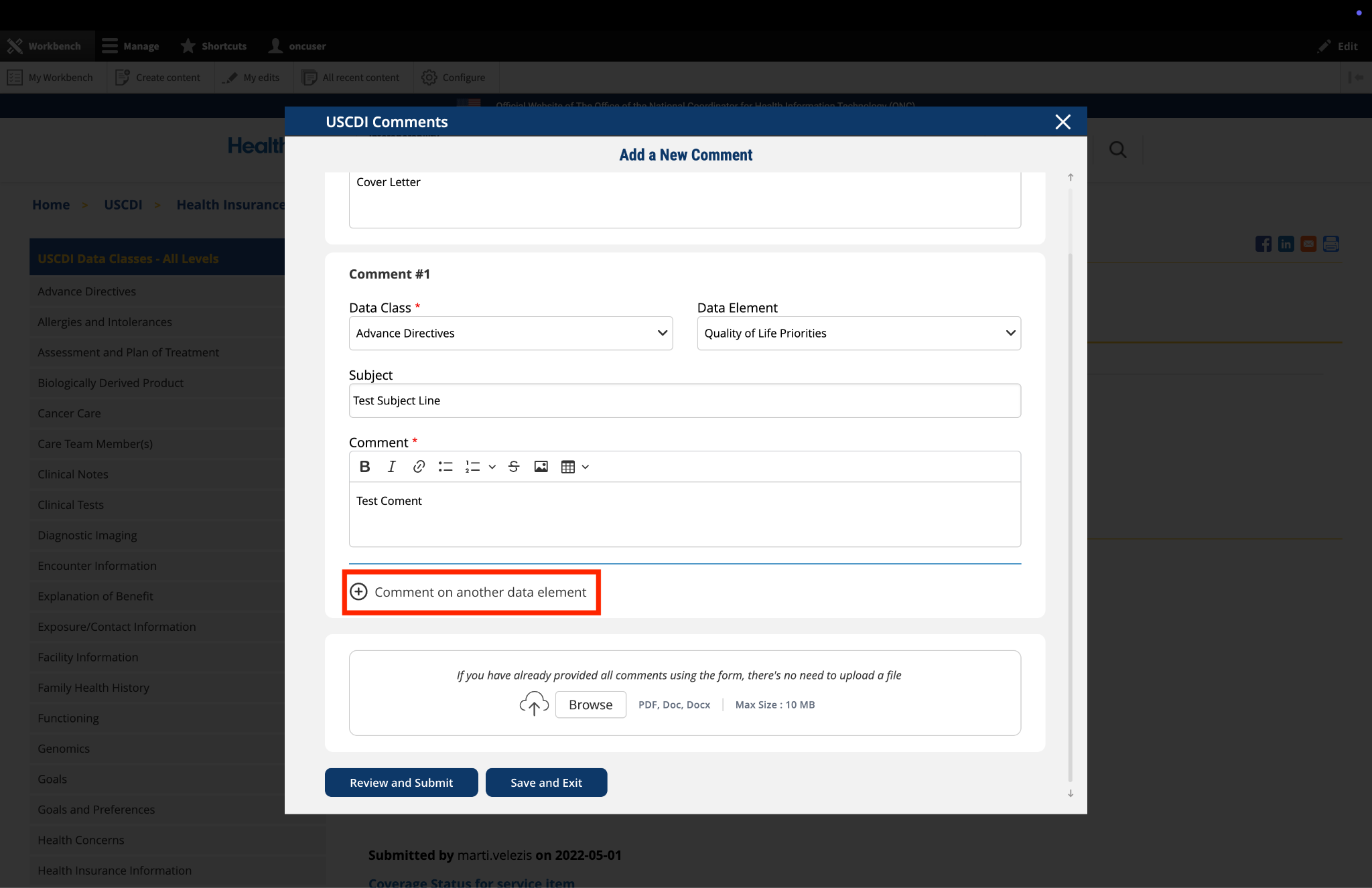
6. Optional: Add Additional Comments
If you need to comment on multiple data classes or elements:
After completing your first comment, click the link labeled "Comment on another data element" at the bottom of the form.
A new comment section will appear, allowing you to enter details for your additional comment.
For each additional comment, you must select the appropriate data class and data element from the drop-down menus.
Complete the Subject and Comment fields for your additional comment.
Repeat this process for each additional comment you wish to submit.
Fig 3 The "Comment on another data element" link enables users to create multiple comments addressing different elements within a single submission.
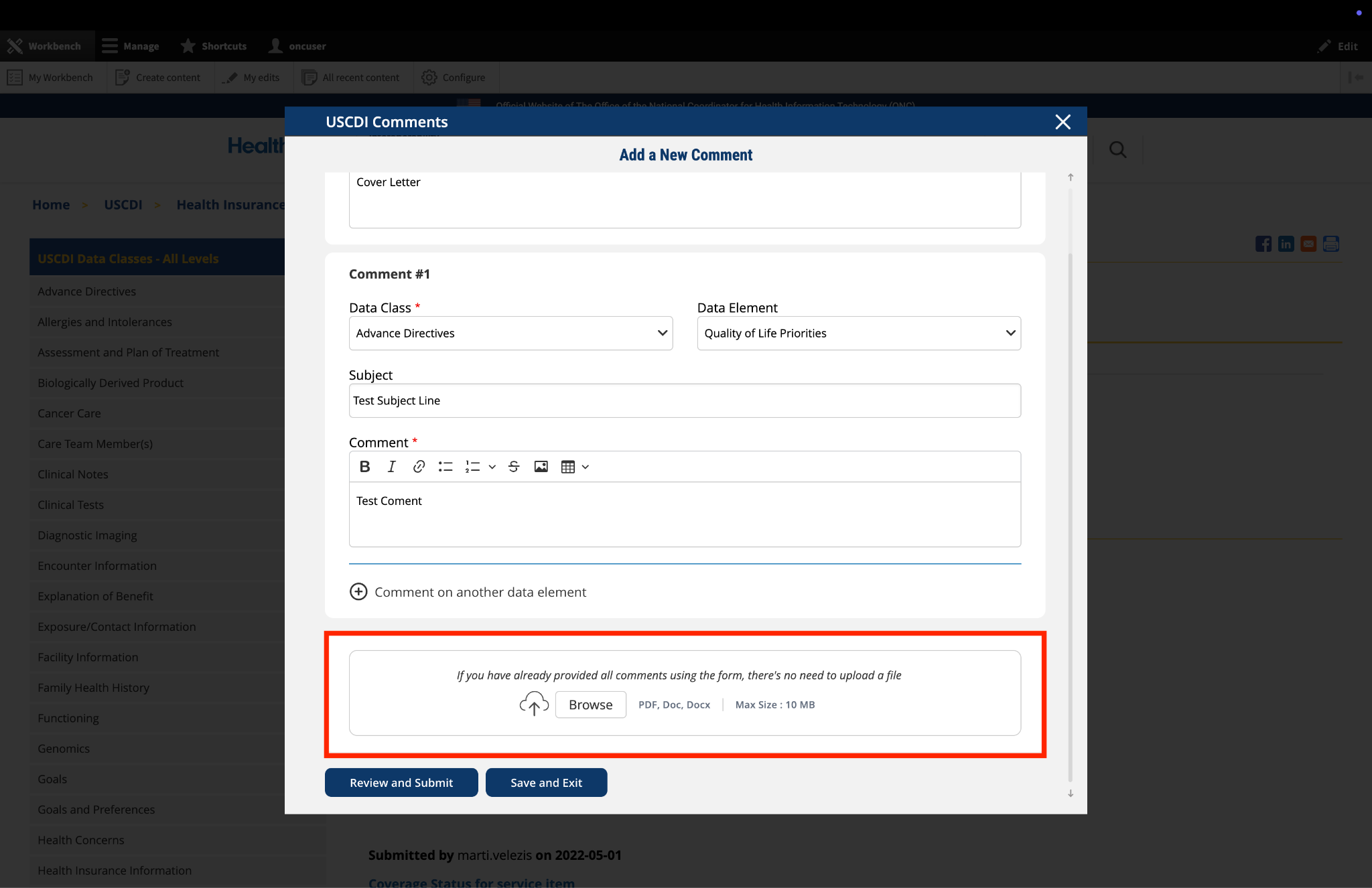
7. Optional: Upload Supporting Files
The platform allows you to upload supporting documentation to enhance your comment:
Locate the "File Upload" section at the bottom of the comment form.
Click to upload any files (such as PDFs or documents) that provide additional context, evidence, or clarification for your comment.
Important: If you have already entered your comments using the form fields, there is no need to upload duplicate content in PDF format. The file upload feature is intended for supplementary materials only. Please avoid uploading files that contain the same information already provided in your comment text.
Fig 4 The "File Upload" section permits users to attach supporting documentation that supplements their written comments.
8. Optional: Save and Exit
If you need to pause your work and return to complete your comment later:
Click the "Save and Exit" button at the bottom of the form.
Your comment will be saved as a draft that you can access and complete later.
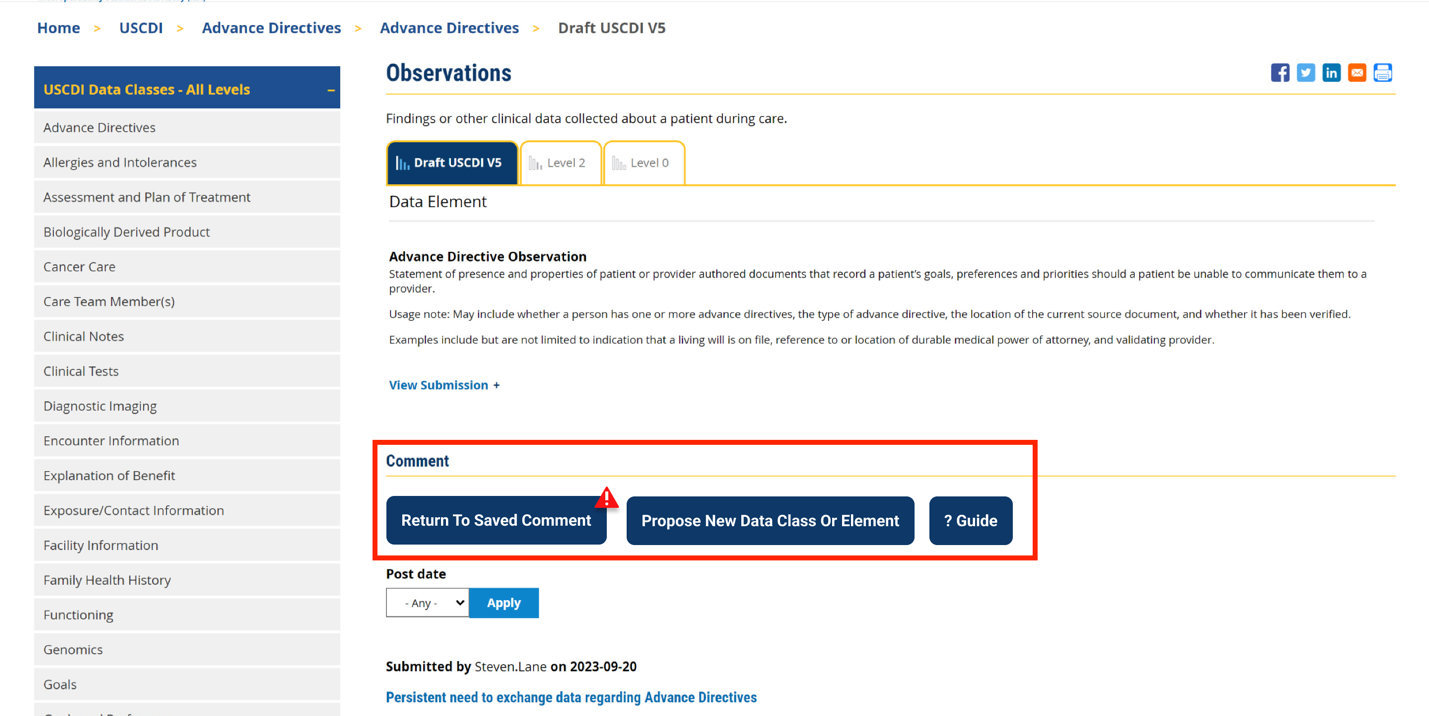
When you return to the platform, you will see a red triangle with an exclamation mark next to the “Return to saved Comment” button, indicating that you have saved comments in draft status.
Click this button to continue working on your draft.
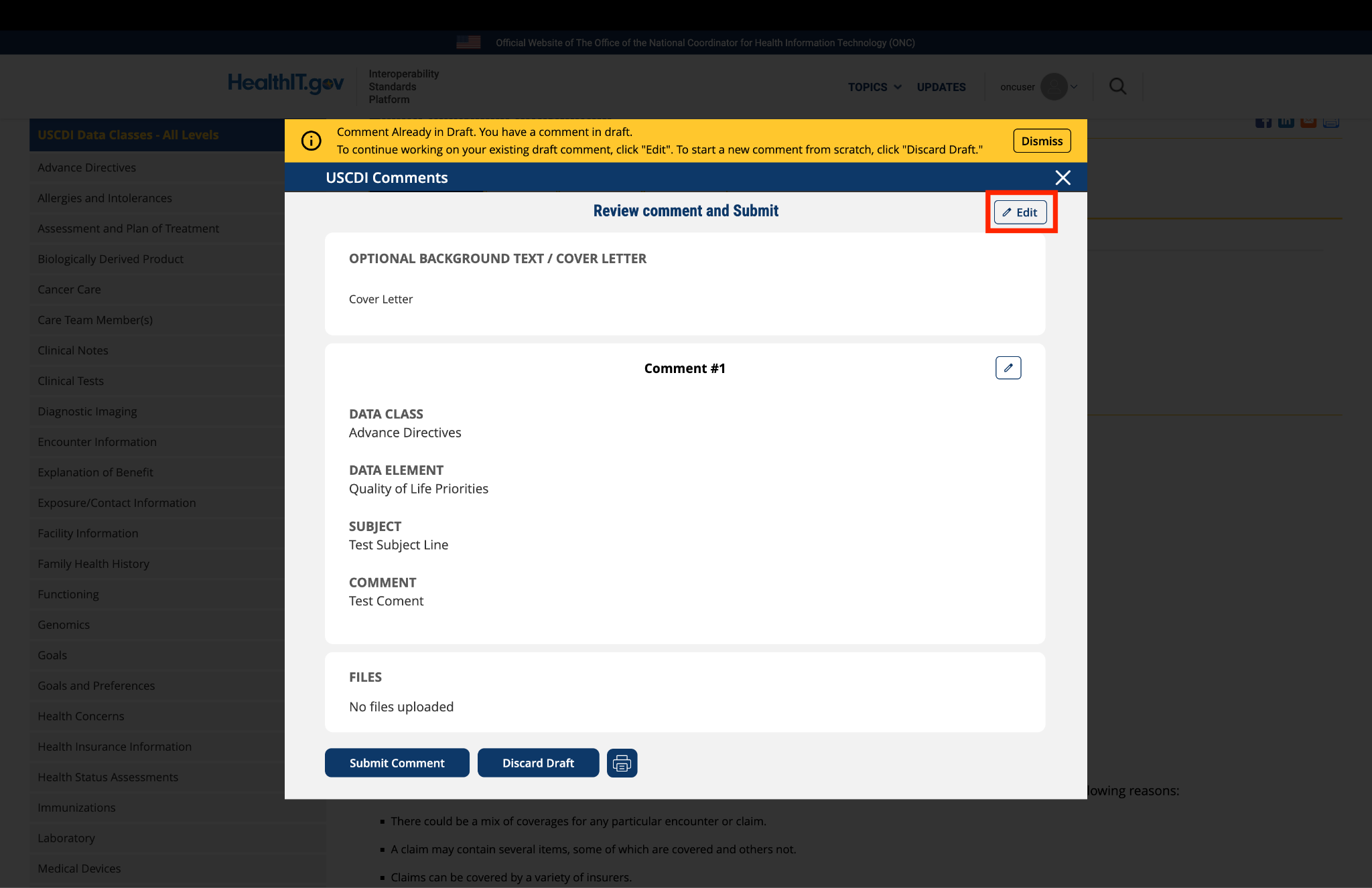
You will be taken to a review page where you can:
Select "Submit Comment" to officially submit your feedback.
Click "Edit" to return to the comment form and make changes
Select "Discard Draft" to delete the saved draft and start fresh
Fig 5 A red triangle with exclamation mark indicator appears next to the “Return to saved Comment” button when draft comments are saved in the system.
9. Review and Submit
Once you have completed your comment:
Click the "Review and Submit" button at the bottom of the form.
This will take you to a review screen displaying your comment(s) in full.
Review all information for accuracy and completeness.
On this review screen, you have three options:
Click "Submit Comment" to officially submit your feedback
Click "Edit" to return to the comment form and make changes
Click "Discard Draft" to delete the comment and start fresh
The review screen also includes a "Print" button that allows you to create a printed copy of your comments for your records.
If you choose to submit, your comment will be recorded in the system and made available for review by the appropriate stakeholders.
Fig 6 The review screen allows users to verify comment content and make any necessary modifications before final submission.

Submitted by amy_rauworth on
Lakeshore LOS for Physical Activity Status to USCDI
Please find attached Lakeshore's letter to express our support for the Physical Activity Alliance's application to add Physical Activity Status as a data element to the next iteration of the US. Core Data for Interoperability (USCDI).
LOS_Lakeshore_ONC_physical activity assessment-Sgned by JDK.pdf