
Official websites use .gov
A
.gov
website belongs to an official government organization in the
United States.
Secure .gov websites use HTTPS
A
lock
(
) or
https://
means you’ve safely connected to the .gov website. Share sensitive
information only on official, secure websites.

Electronic Health Record Adoption and Exchange Capabilities Among Substance Use and Mental Health Treatment Facilities, 2024
April 2026
In recent years, rising prevalence of behavioral health disorders has led to increasing demand for substance use and mental health treatment services.(1) Electronic health record (EHR) use is critical to improving clinical care, quality of care, and patient outcomes, as well as facilitating the exchange of health information.(2) While EHR adoption is nearly universal among hospitals and physicians, data remains limited regarding the adoption of EHRs and health information exchange capabilities among substance use and mental health treatment facilities.(3) Using data from the 2024 National Substance Use and Mental Health Services Survey (N-SUMHSS), administered by the Substance Abuse and Mental Health Services Administration (SAMHSA), this data brief examines the adoption and exchange capabilities among substance use and mental health treatment facilities in the United States. Results can help inform efforts to advance the adoption and use of health IT in behavioral health settings.
Highlights
- More than two-thirds of substance use and mental health treatment facilities (facilities) only used an electronic health record (EHR) – no paper charts – to maintain patient records, which varied by ownership type.
- Facilities used EHRs for the same core tasks—recording patient health information and monitoring patient progress—at similar rates, regardless of whether they used an EHR only or used a combination of an EHR system and paper charts.
- Fewer facilities reported using an EHR for exchanging health information, care coordination, and patient engagement than for recording patient health information.
- One in five facilities reported participating in a health information exchange organization (HIE); HIE participation was associated with substantially higher frequencies of searching and querying for patients’ health information compared to non-participants.
More than two-thirds of facilities only used an electronic health record (EHR) to maintain patient records, which varied by ownership type.
Findings
- Compared to private for-profit organizations (68%), EHR adoption was significantly higher among federal government facilities (97%) and local, county or community government facilities (73%) and significanly lower among state government facilities (38%).
- 1 in 4 facilities reported using a combination of an EHR system and paper charts to maintain patient records, however, this varied by ownership type. Rates of using a combination of EHR and paper charts were highest among state government facilities (51%), while the lowest rates were reported among private for-profit organizations (22%) and federal government facilities (3%).
- Few facilities (4%) reported they had no plans to implement an EHR.
Figure 1: Percent of substance use and mental health treatment facilities that used EHRs or paper charts by ownership, 2024
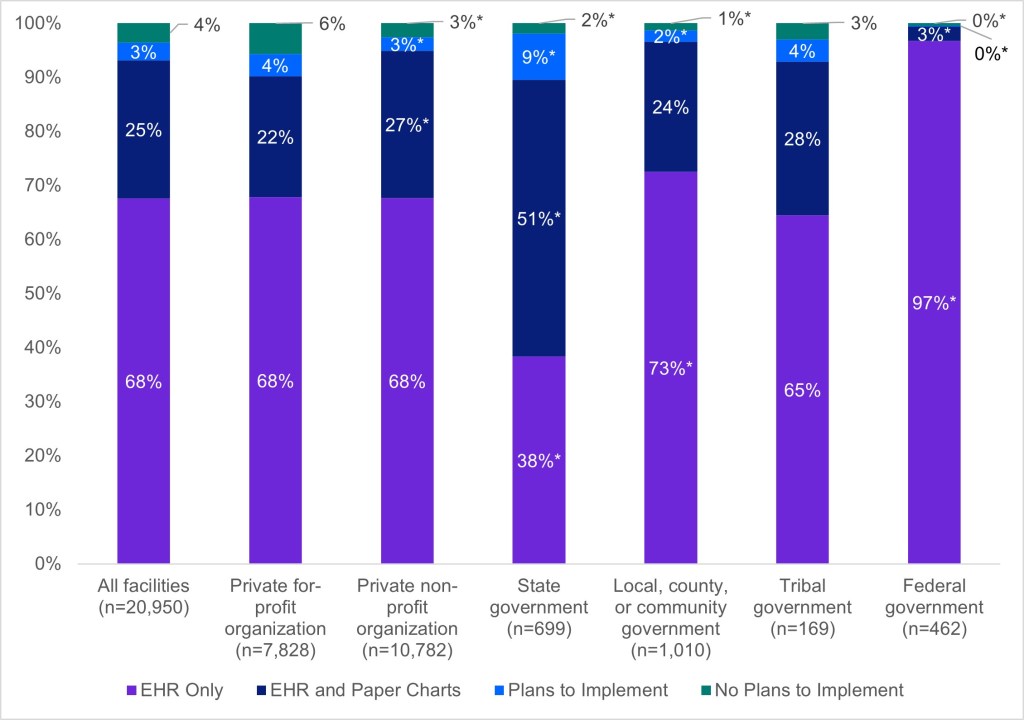
Notes: n=20,950; missing responses were excluded from the denominator. *Indicates statistically significant difference relative to the reference group (private for-profit organization) (p<.05). See the Definitions section for definition of terms.
Facilities used EHRs for the same core tasks—recording patient health information and monitoring patient progress—at similar rates, regardless of whether they only used an EHR or used a combination of an EHR system and paper charts.
Findings
- Facilities reported near universal use of an EHR to record patient information and monitor patient progress, with slightly higher rates among facilities that only used an EHR compared to those that used a combination of an EHR system and paper charts.
- Among facilities who used a combination of EHR and paper charts, 84% reported using an EHR to record referrals, nine percentage points less than facilities who reported only using an EHR.
Table 1: Percent of substance use and mental health treatment facilities that used EHRs to record patient health information by facility EHR adoption (EHR only vs EHR and paper chart use), 2024
| Used an EHR to… | Facilities that only use an EHR (68%) | Facilities that use both an EHR and paper charts (25%) |
|---|---|---|
| Record patient demographic information | 99% | 98%* |
| Record diagnoses | 99% | 98%* |
| Record clinical or progress notes | 100% | 97%* |
| Record patient history | 100% | 97%* |
| Monitor client progress | 99% | 96%* |
| Record treatment plans | 99% | 94%* |
| Record discharge plans | 99% | 95%* |
| Record behavioral health screenings or tools | 99% | 92%* |
| Record patients’ medications | 98% | 92%* |
| Record problem lists | 98% | 93%* |
| Record patients’ allergies | 98% | 92%* |
| Record social determinants of health (employment, housing) | 96% | 92%* |
| Record referrals | 93% | 84%* |
Notes: Missing and “not applicable” responses were excluded from the denominator. *Indicates statistically significant difference relative to the reference group (EHR only) (p<.05). See the Definitions section for definition of terms.
Fewer facilities reported using an EHR for exchanging health information, care coordination, and patient engagement than for recording patient health information.
Findings
- Facilities that only used an EHR reported substantially higher rates of using an EHR for exchanging health information, care coordination, and patient engagement than those that used a combination of an EHR system and paper charts.
- The largest gaps for EHR use between facilities that only used an EHR and those that used a combination of an EHR system and paper charts were for ordering lab tests and sending prescriptions to pharmacies.
Table 2: Percent of substance use and mental health treatment facilities that used EHRs to exchange health information, coordinate care, and engage with patients by facility EHR adoption (EHR only vs EHR and paper chart use), 2024
| Used an EHR to… | Facilities that only use an EHR (68%) | Facilities that use both an EHR and paper charts (25%) |
|---|---|---|
| Exchange Health Information | ||
| Integrate outside information electronically | 48% | 36%* |
| Send prescriptions | 82% | 62%* |
| Search or query | 56% | 53%* |
| Care Coordination | ||
| Review warnings or alerts | 87% | 72%* |
| Reconcile medications | 84% | 69%* |
| View lab results | 78% | 61%* |
| Order lab tests | 71% | 50%* |
| Check PDMP | 72% | 57%* |
| Patient Engagement | ||
| View medical record online | 44% | 33%* |
| Secure messaging | 45% | 33%* |
Notes: Missing and “not applicable” responses were excluded from the denominator (except for search or query and integration without manual entry, as “not applicable” was not a response option). *Indicates statistically significant difference relative to the reference group (EHR only) (p<.05). See the Definitions section for definition of terms.
One in five facilities reported participating in a health information exchange organization (HIE), with about two-thirds of facilities reporting no knowledge or familiarity of one in their service area.
Findings
- 19% of facilities reported participating in an HIE, while the majority of facilities (67%) reported they were not familiar with an HIE or did not know about HIE availability in their service area.
- Few facilities (7%) reported not participating in available HIEs in their service area.
Figure 2: Participation in state, regional, and/or local Health Information Exchange Organization (HIE), 2024
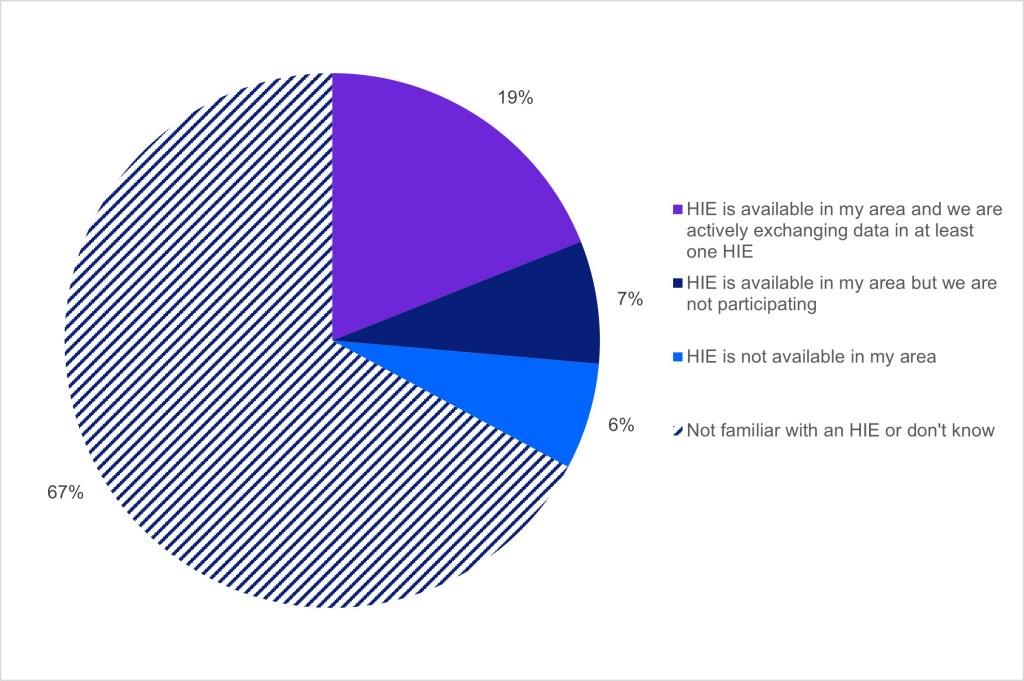
Notes: n=19,485; missing responses were excluded from the denominator. See the Definitions section for definition of terms.
HIE participation was associated with substantially higher rates of searching and querying for patients’ health information and HIE participants were less likely to report no capability compared to non-participants.
Findings
- Among the 19% of facilities that participated in an HIE (Figure 2), 44% reported electronically searching or querying for health information every day, compared to 25% of facilities who did not participate in an HIE.
- Half of the facilities that did not participate in a HIE reported never searching or querying for patient health information or not having the capability to do so. Fewer than 1 in 4 HIE participants reported the same.
Figure 3: Frequency of electronically searching or querying for patients’ health information from other providers or external sources, 2024
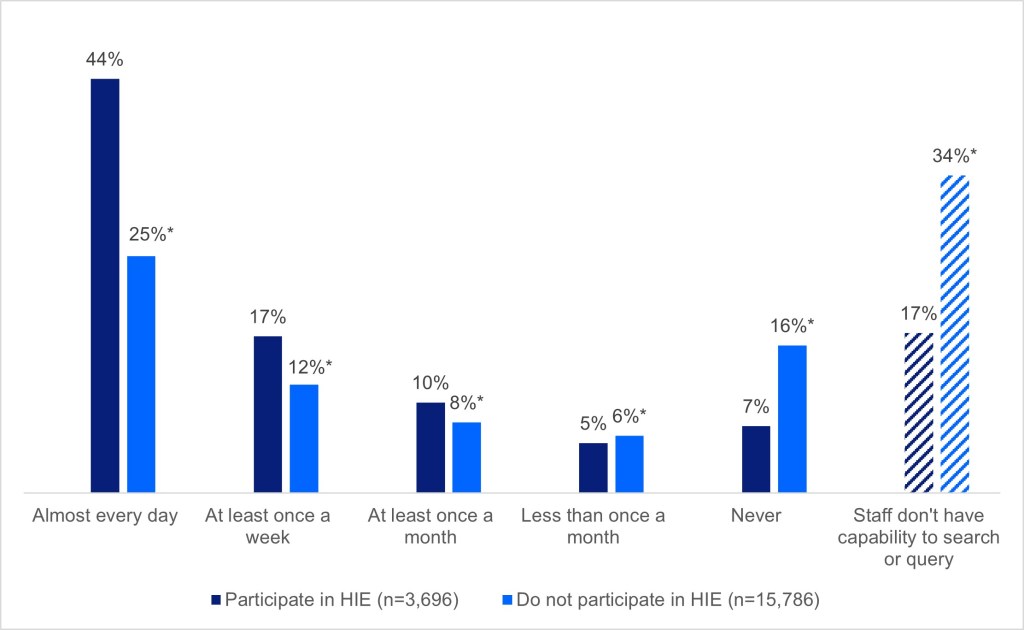
Notes: n=19,482; missing responses were excluded from the denominator. *Indicates statistically significant difference relative to the reference group (participate in HIE) (p<.05). See the Definitions section for definition of terms.
Summary
Advances in health information interoperability have highlighted the need for greater adoption of EHRs to support care coordination and facilitate data sharing between health care providers and substance use and mental health treatment facilities.(4) Historically, behavioral health facilities have lagged behind non-federal acute care hospitals in health IT capabilities.(5) The 2009 Health Information Technology for Economic and Clinical Health (HITECH) Act largely focused on providing incentive payments to eligible hospitals and health care professionals to adopt and use certified EHRs, which excluded substance use and mental health treatment facilities.(3) As a result, EHR adoption and interoperability gaps persist.
In this brief, we examined current adoption and exchange capabilities of EHRs among substance use and mental health treatment facilities. In 2024, more than two-thirds of facilities only used EHRs (no paper charts), while few facilities reported they had no plans to do so (4%) (Figure 1). Studies have found that key barriers to EHR adoption include the lack of financial incentives for behavioral health clinicians, privacy concerns related to the sharing of patient information, staffing capacity, provider burnout, and the lack of available resources to maintain information technology infrastructure.(3) Our analysis showed that EHR adoption rates varied by facility ownership (Figure 1). Facilities operated by the federal government (predominantly operated by U.S Department of Veterans Affairs) had the highest rates of EHR adoption (97%). Adoption rates were similar among facilities operated by private for-profit organizations (68%), private non-profit organizations (68%), and tribal governments (65%). However, adoption rates were lowest among facilities operated by state governments (38%), indicating a significant gap possibly due to cost, data fragmentation, and workforce challenges.
The survey data also showed that the use of the EHR for various clinical and administrative tasks varied among facilities. Overall, we found that fewer facilities reported using an EHR for exchanging health information, care coordination, and patient engagement than for recording patient health information (Table 1, Table 2). Facilities that only used an EHR were more likely to record patient information, exchange information electronically, and coordinate care via the EHR than those facilities that also used paper charts. However, the gap varied by the type of task. Whereas facilities only using an EHR were more likely to use an EHR to record information, the gap was small compared to facilities that used a combination of EHR and paper charts (less than 10 percentage points). However, for other tasks like sending prescriptions and ordering or viewing lab results, the use of the EHR was overall lower for all facilities and there was a wider gap between facilities that only used an EHR and those that used both an EHR and paper charts (Table 1, Table 2). The data suggest that there may be both gaps in the capabilities of implemented EHRs to perform certain tasks and gaps in how some facilities implemented and used their EHR, perhaps using computer-based tools outside their EHR workflow, other non-EHR methods, or paper-based practices for some tasks versus others.
Our findings demonstrate that while most behavioral health facilities use an EHR system and there is near universal adoption of using an EHR to record patient information among EHR users, potential interoperability and technology challenges may limit behavioral health data exchange. Factors such as technical barriers, workforce, cost, and privacy concerns may contribute to lower electronic exchange of health information.(3, 6, 7) We found that 56% of facilities at least sometimes electronically searched for patient health information and that this did not vary much between facilities that only used an EHR and those that used a combination of an EHR and paper charts (Figure 3). The data also show that 19% of facilities reported participating in a health information exchange organization (HIE) with 67% reporting no knowledge or awareness of one in their service area (Figure 2). We found a clear relationship between a facility’s participation in a HIE and their capability and frequency to electronically search or query for health information. Six in ten facilities that participated in an HIE reported searching for patient health information daily or weekly, while fewer than four in ten non-HIE facility participants did the same. Greater access to and integration with health information networks may advance facilities’ interoperability capabilities and better connect them with other providers who care for shared patients. To address these challenges, several states have recently developed innovative solutions to support interoperability, including the Health Care Management and Coordination System in Washington state, aimed at improving data sharing across multiple state agencies and care settings.(5)
In response to the increasing demand for behavioral health care, several federal agencies are working together to develop initiatives aimed at improving EHR adoption rates and behavioral health data exchange. HHS Secretary Kennedy, together with the Office of the National Coordinator for Health IT (ONC) and SAMHSA, recently announced the selection of nine nationwide pilot programs to test health IT standards.(8) This pilot program is funded through a larger Behavioral Health Information Technology (BHIT) Initiative.(9) The program includes 45 exchange partners across nine states and findings will help inform standards and policy considerations. The pilot projects will identify effective practices and opportunities that can support improved behavioral health data exchange for patients and providers. Other ONC initiatives include the Behavioral Health eCarePlan Collaborative Project, which seeks to adapt an open-source application for three behavioral health use cases and pilot it in clinics that face challenges with exchanging health information.(10) Continued efforts to address behavioral health data exchange challenges are critical to improve the continuity of care and improve health outcomes. Under the Support Act Reauthorization, ONC is also convening a public roundtable to examine how to use health information technology to improve mental health and substance use care outcomes and preparing a subsequent report to Congress by the end of 2026.(11)
Definitions
Check PDMP: The EHR’s capability to check state’s prescription drug monitoring program (PDMP) prior to prescribing a controlled substance.
Electronic health records (EHRs): For the purpose of the survey, EHRs are an electronic version of a patient’s medical history that is maintained by the provider over time and may include all of the key clinical data relevant to that person’s care under a particular provider. These do not include billing record systems.
EHR only: Substance use or mental health treatment facilities that exclusively used an EHR system. No paper charts.
Health Information Exchange Organization (HIE): A Health Information Exchange Organization (HIE) is an organization that oversees and governs the exchange of health-related information among organizations according to nationally recognized standards.
Integrate outside information electronically: The EHR’s capability to integrate clinical information received electronically from outside providers, without manual entry.
Market leading EHR developers: Market leading EHR developers by market share. The market share is based on substance use and mental health treatment facilities’ responses to the 2024 survey.
Order lab results: The EHR’s capability to order lab results.
Ownership: Respondents were instructed to select one of six possible responses: private for-profit organization; private non-profit organization; state government; local, county, or community government; tribal government; and federal government.
Paper charts: All non-electronic resources used to accomplish work associated with a clinical, administrative or information management activity. Non-electronic resources include e-fax, pdf, or scanned documents. These are considered paper documents.
Patient: A person receiving treatment at a substance use or mental health treatment facility. Patients are also referred to as clients and the terms are used interchangeably in the 2024 N-SUMHSS survey.
Reconcile medications: The EHR’s capability to reconcile medications when admitting, discharging, and/or transitioning clients between care settings.
Review warnings or alerts: The EHR’s capability to review warnings or alerts of medication allergies, drug-drug interactions or contraindications.
Secure messaging: The EHR’s capability to allow patients to exchange secure messages with staff.
Send prescriptions: The EHR’s capability to electronically send prescriptions to the pharmacy.
Search or query: The EHR’s capability to electronically search or query for patients’ health information from other providers or external sources.
Substance use and mental health treatment facilities: Facilities in the United States, both private and public, that provide services to diagnose, treat, or support individuals with substance use disorders and/or mental health conditions, including inpatient, residential, and outpatient levels of care.
View lab results: The EHR’s capability to view lab results.
View medical records online: The EHR’s capability to allow patients to view their medical record online.
Data Sources and Methods
Data are from the 2024 National Substance Use and Mental Health Services Survey (N-SUMHSS). The 2024 survey was conducted from March 29, 2024, through December 9, 2024. The N-SUMHSS collects data annually on the location, characteristics, and utilization of substance use and mental health treatment facilities. The data collected provide a mechanism to quantify the diverse characteristics and composition of substance use and mental health treatment delivery systems across the United States, the District of Columbia, and U.S. territories. The Center for Behavioral Health Statistics and Quality (CBHSQ) at SAMHSA, U.S. Department of Health and Human Services, plans and directs the N-SUMHSS.
The 2024 N-SUMHSS was conducted using a multimode data collection approach that included: (1) a secure web-based survey, (2) a postal paper survey, and (3) computer-assisted telephone interviews (CATI). Of the 27,957 treatment facilities known to SAMHSA in 2024, 23,948 were deemed eligible to participate in the survey. Among these, 21,205 unique facilities completed the survey, yielding a robust overall response rate of 90.4%. Facilities were categorized as providing substance use treatment, mental health treatment, or both substance use and mental health treatment. Because many facilities offer multiple types of services, facility counts and percentages are not mutually exclusive. Data was collected from 15,953 substance use treatment facilities, 14,091 mental health treatment facilities, and 8,839 combined substance use and mental health treatment facilities. In the 2024 survey, all substance use and mental health facilities were asked to complete questions regarding electronic health records, including topics like EHR use and satisfaction, network participation, interoperability, patient engagement.
Data Availability
The National Substance Use and Mental Health Services Survey (N-SUMHSS) data are publicly available from SAMHSA: https://www.samhsa.gov/data/data-we-collect/n-sumhss-national-substance-use-and-mental-health-services-survey/annual-releases/2024. If you have questions or would like to learn more about the data source or these findings, you may contact ONC_Data@hhs.gov.
References
- National Academies Press. In: Perera U, Godwin A, Polsky D, editors. Expanding Behavioral Health Care Workforce Participation in Medicare, Medicaid, and Marketplace Plans. Washington (DC)2024.
- Frimpong JA, Liu, X., Liu, L., Zhang, R. Adoption of Electronic Health Record Among Substance Use Disorder Treatment Programs: Nationwide Cross-Sectional Survey Study. J Med Internet Res. 2023;25:e45238.
- Dougherty M, McGavin, M., Pilar, M., Horvath, M., & Brown, S. Health Information Technology Adoption and Utilization in Behavioral Health Settings (Final Report). Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health and Human Services; 2024.
- Jung SY, Hwang, H., Lee, K., Lee, D., Yoo, S., Lim, K., Lee, H. Y., Kim, E. User Perspectives on Barriers and Facilitators to the Implementation of Electronic Health Records in Behavioral Hospitals: Qualitative Study. JMIR Form Res. 2021;5(4):e18764.
- Lubell J. Health IT Advances for Behavioral Health Bring New Challenges to HI Professionals. Journal of AHIMA [Internet]. 2024. Available from: https://journal.ahima.org/page/health-it-advances-for-behavioral-health-bring-new-challenges-to-hi-professionals.
- Shank N. Behavioral health providers’ beliefs about health information exchange: a statewide survey. J Am Med Inform Assoc. 2012;19(4):562–9.
- Cochran RA, Feldman SS, Ivankova NV, Hall AG, Opoku-Agyeman W. Intention to Use Behavioral Health Data From a Health Information Exchange: Mixed Methods Study. JMIR Ment Health. 2021;8(5):e26746.
- ASTP/ONC Announces Selection of Nationwide Pilot Programs to Improve Behavioral Health Data Exchange [press release]. 2026.
- Chickasaw Federal Health. Pilot Program for Behavioral Health Data Exchange Partners Behavioral Health Information Technology (BHIT) Pilot Program [Available from: https://www.chickasaw.com/USCDI-BH-Pilot-Program.
- Office of the National Coordinator for Health IT (ONC). 2024 LEAP in Health IT Projects 2026 [Available from: https://healthit.gov/interoperability/investments/leap/2024-leap-health-it-projects/#behavioral-health-ecareplan-collaborative-project.
- SUPPORT for Patients and Communities Reauthorization Act of 2025, 119th Congress (2025-2026)(2025).
Acknowledgments
The authors are with the Office of Standards, Certification, and Analysis, within the Office of the National Coordinator for Health IT (ONC). The data brief was drafted under the direction of Mera Choi, Director of the Technical Strategy and Analysis Division, Vaishali Patel, Deputy Director of the Technical Strategy and Analysis Division, and Wesley Barker, Chief of the Data Analysis Branch with subject matter expertise from Samuel Kaardal and Mitch Chaney.
Suggested Citation
Chang W, Owusu-Mensah P. Electronic Health Record Adoption and Exchange Capabilities Among Substance Use and Mental Health Treatment Facilities, 2024. Office of the National Coordinator for Health IT. Data Brief: 82. April 2026.
Appendix
Appendix Table A1: Market leading EHR developers among substance use and mental health treatment facilities, 2024
| n | % | |
|---|---|---|
| Qualifacts/Credible (CareLogic EHR) | 2,277 | 11.7% |
| Netsmart (MyAvatar, MyEvolv) | 2,052 | 10.5% |
| EPIC | 1,300 | 6.7% |
| Methasoft (Netalytics) | 686 | 3.5% |
| NextGen | 598 | 3.1% |
| Cerner | 552 | 2.8% |
| E-Clinical Works (ECW) | 439 | 2.3% |
| SAMMS | 221 | 1.1% |
| Meditech | 206 | 1.1% |
| Ten Eleven | 193 | 1.0% |
| Welligent | 187 | 1.0% |
| Other | 11,024 | 56.5% |
Notes: n=19,514 (includes all 24 response options, don’t know, and other); missing responses were excluded from the denominator.